
During a Utah in the Weeds podcast from late 2020, hosts Tim and Chris welcomed guest Desiree Hennesey from Utah Patients Coalition, with strong legislative ties in hopes of talking about what's going on with Medical Cannabis at the state level. They learned of an effort to change the law so that any licensed doctor in the state can prescribe Medical Marijuana without having to go through the process to become a Qualified Medical Provider (QMP).
What do you think? Should any doctor be able to write your prescription? There are a lot of people that think so. Loosening up the QMP requirements might even convince some doctors still on the fence to climb over into the greener fields of Medical Cannabis. Would this help or hurt patients across the state?
Those in favor of the rule changes suggest that allowing all doctors to prescribe would:
Proponents want patients to have easy access to Medical Marijuana, but should Medical Cannabis be as easy to get as penicillin? That is what it boils down to.
Right now, almost 600 of Utah's doctors, PAs and NPs are registered Qualified Medical Providers, allowed by the state of Utah, to recommend Medical Marijuana to their patients. These providers have completed 4 hours of specialized training and registered with the Department of Health in order to make these recommendations. Doctors who are not registered, and are not QMPs, stay away from Medical Marijuana for plenty of reasons. Some do not think it is worth their while. Others are afraid they don't know enough about cannabis. Some still aren't sure where they stand in terms of liability.
Right now, the majority of Medical Providers actively working with patients are located in the Provo and Salt Lake areas. If you live in rural Utah, you could end up driving quite a distance just to see a Medical Cannabis specialist. You might have to drive to get to a dispensary now, too. But as more dispensaries open, wouldn't it be nice if there were more doctors helping patients get their Medical Cannabis cards? More participating doctors means less travel for a lot of patients.
There is another aspect to the legislation that deserves some serious consideration. It has been proposed that the state allow any licensed doctor to assist patients in obtaining a Medical Cannabis card, with or without QMP training. But when it comes time to write an actual recommendation, the task will be left to a Medical Cannabis pharmacist.
This sort of thing is risky in a number of ways.
If all the doctor is required to know is that the patient sitting in their office legitimately suffers from a qualifying medical condition, it’s only half the job. The second half is evaluating what treatment options are best for that patient and recommending the best possible options. Though we would not necessarily expect a medical provider to fully understand cannabis and the cannabinoid system, we would expect the doctor to know at least what the main benefits and risks are, the legal implications for their patient, and how to educate their patient on those things.
It is a pharmacist’s job to understand drugs and how they affect patients. This makes a pharmacist a great source of information and education for Medical Cannabis patients. But the idea of allowing all doctors to be a Qualified Medical Provider and to recommend Medical Cannabis to patients and leaving all the work to the pharmacist is potentially risky for doctors and could be risky for patients.
So. should all doctors in the state of Utah be allowed to prescribe Medical Marijuana? Some people think so. And if they have their way, the rules in Utah could be changed this year.
Utah in the Weeds Episode 52 features a fascinating discussion with two hemp growers named Josh and Derrick. They are friends who met through their shared appreciation of disc golf. Josh's background is in plant biology where Derrick's is in the medical side of things. Between them, they run two businesses: Uinta Cannabis in Utah and Utah Hemp Growers based in Nevada.
Uinta Cannabis was the first company formed. During the conversation, the partners revealed that Josh had the idea to become a grower first. After talking to a lot of people but not finding any interest, he met Derrick. They came up with a viable business plan and recruited investors.
The idea for the Utah Hemp Growers marketplace was born out of a desire to sell raw flower. The partners were able to initially do so, but then Utah law changed. Now they have to sell from Nevada. Incidentally, their Nevada company only sells hemp products produced by Utah growers.
Josh and Derrick discussed the many hoops they have to jump through to make their business work. For starters, they had to secure a lease before they could even apply for a license. Since then, they have gone to great lengths to maintain regulatory compliance.
Josh and Derrick also spent time discussing their philosophy of focusing on product experience rather than chasing specific cannabinoid profiles. They explained that experience is more important because people react to profiles differently. It is an interesting approach that Tim and Chris seemed to warm to as they listened to the explanation.
Episode 52 is the latest in a line of interviews from business owners actively on the ground. If you are interested in what it takes to get hemp to market, this is a conversation for you.
More Information Coming Soon...
Follow the podcast at UtahMarijuana.org, or leave us a message at (385) 215-9557.
Check out Chris Holifield’s other podcast, I am Salt Lake.
Subscribe to our YouTube Channel, Discover Marijuana.
Chris:
All right, let's welcome everybody out today to episode 52 of Utah in the Weeds. How are you doing today, Tim?
Tim:
I'm doing good, Chris. I'm excited for episode 52 in this conversation with these two guys with some military background, right?
Chris:
Yeah, Josh and Derrick from Utah Hemp Growers and Uinta Cannabis. They got a fantastic story of kind of how they started growing hemp and how it kind of evolved into this business selling other Utah hemp farmer’s hemp basically to people here in Utah.
Tim:
Right, created a marketplace because there really wasn't one for their products and a good discussion about the intricacies, again, of this getting into the hemp growing space and what you have to do to sell smokable flower in Utah and some of those technicalities. I thought the biggest takeaway for me, Chris, with this interview was that sometimes more regulation is better.
Chris:
Yeah, exactly.
Tim:
Right, because there's clear ... There's a clearer pathway to your business model and to getting people the products that they need.
Chris:
Yeah, no, I think our listeners are going to love this conversation. I was actually really excited after we finished recording. I'm like I can't wait to get this up for everybody to listen to. So make sure you stick around for the whole conversation. We're going to get into that here in just a minute. Utahmarijuana.org/podcast is where you can listen to all the podcast episodes. Make sure you're sharing them with your family and friends because that's how we get the word out about the podcast. Is there anything going on, anything new, with you, Tim, going on that you need to share with our listeners?
Tim:
I mean here we come up, this will be the first episode in April and 4/20 is going to come up. We have Earth Day. We'll be announcing some service that we want to do through utahmarijuana.org in the next couple of weeks, so stay tuned for the next episodes on that. Yeah, I mean this is just an exciting month. It's the celebratory month-
Chris:
Yeah, 4/20, baby!
Tim:
Right.
Chris:
We finally got a 4/20 that we can celebrate and hopefully, I want to have some good episodes this month. Well, we got good episodes every week. So make sure to subscribe-
Tim:
You ought to stay tuned.
Chris:
... in whatever podcast app you listen to. We got a brand new episode every week, 4:20 a.m. on Friday. Let's get into that episode with Josh and Derrick from Uinta Cannabis and Utah Hemp Growers.
Tim:
All right, enjoy everybody.
Chris:
Thanks for listening.
Tim:
Yeah, I mean here we are with Josh and Derrick. I mean how did you guys meet?
Josh:
Well, I had had the idea for getting a grow started for quite some time and I had gone through quite a few people with the idea, saying, "Hey, I'm thinking about starting up a cannabis grow," and most people were kind of under that assumption of just like oh yeah, you want to grow free weed, whatever.
Tim:
Right, of course.
Josh:
And so, it was actually-
Tim:
And it was popular like when are you having these conversations?
Josh:
I mean I had approached some family and friends with a legitimate business plan saying, "Hey, I want to get this going," and there was the initial excitement and then it would fizzle out into nothing-
Tim:
Right.
Josh:
... and so-
Tim:
You're like wow, this is so great. We're going to grow cannabis.
Josh:
Yeah, and I'm like okay, but this is a serious business. We're going to be farmers. It's work every day and so approaching people, it would just ... Like I said, just fizzle out and I actually approached Derrick about it, just in passing conversation at our little disc golf group and he actually showed interest and so we got to talking about it and then we thought up a business plan and started drafting up ideas and started raising capital and just went from there.
Chris:
Wow. How did the two of you even meet?
Josh:
Through common friends.
Chris:
Through common friends? Okay.
Josh:
Yeah, yeah, through kind of a disc golf crew-
Chris:
Disc golf. Man, that's one of those things I need to learn how to-
Josh:
Oh, it's fantastic.
Chris:
I hear from everybody about how much fun that game is and I've never played.
Tim:
It is a fun game and there is nowhere you have to pay for it, right?
Josh:
No, it's free.
Tim:
It's free everywhere you play.
Josh:
Yeah, except-
Tim:
There's a cool course in West Bountiful that I've played at. There used to be a course up at the University of Utah but I think they've taken most of it down?
Derrick:
Yeah, that was a free course. Yeah, I think they took a good portion of it down. I play mainly at Creekside. So it's free-
Tim:
Oh, okay.
Derrick:
It's beautiful. It's like one of the first 50 courses in the entire country. It's great.
Tim:
I think if you just show up and throw a disc, I mean that's my experience, right?
Josh:
Yeah, you can show up and start on hole four and play through hole nine and walk out, so yeah.
Tim:
Okay, well-
Josh:
I still suck at it.
Tim:
Yeah, well.
Chris:
So, what came first, Uinta cannabis or Utah Hemp Growers. I would imagine Uinta Cannabis came first…
Josh:
Uinta Cannabis came first. That was thought up beginning of 2019 and we got serious about it early fall, raised the capital that we needed from some friends and family and our life savings, both of ... Just all the money that we had and so we filed for the permits and-
Chris:
Was it tough to file for all that? I mean were there obstacles? I mean this is Utah we're talking about here.
Derrick:
Oh, wow, yeah, obstacles.
Josh:
The biggest obstacle by far was that the law required us to have a location locked in before we could file for our grow license, which kind of sucked because-
Chris:
So, you had to have a leased signed? You had to sign a lease almost-
Josh:
Correct.
Chris:
... get into debt and not even be guaranteed-
Josh:
… before we could get a grow license.
Derrick:
Correct.
Tim:
Yeah, how does the landlord look at that? He's like you've signed a lease, you're hooked.
Josh:
Yeah, so-
Tim:
Whether you get a permit or not.
Josh:
Yeah, exactly. We went through-
Tim:
Right, you're going to grow potatoes, you're going to grow cannabis.
Josh:
Yeah, we went through about 15 different locations of people not calling us back-
Derrick:
Flat out saying no.
Josh:
... stringing us along. The second that you mention cannabis, they're just like nope, we want nothing to do with that.
Derrick:
No, thank you.
Tim:
What year is this that you're-
Josh:
2019.
Derrick:
Yeah.
Tim:
Oh my gosh, this is so recent.
Josh:
Yes.
Derrick:
Yes.
Tim:
But this is during the time when ... And we've talked to quite a few guests about this, the time when CBD oil and biomass is still profitable.
Josh:
Yeah, one acre was like $150,000.
Derrick:
Yeah, ridiculous. Yeah.
Tim:
You were right at the end.
Josh:
Green rush.
Tim:
I mean you were getting into the business right before it just-
Josh:
Well, I saw ... I saw the writing on the wall-
Tim:
... crushes you.
Josh:
... that everyone's going to jump in. People are going to jump in that have never touched cannabis and the markets going to-
Tim:
Or never been farmers.
Josh:
... or never been farmers and it's going to inflate it and crash it and look what happened.
Tim:
Wow.
Josh:
Yeah.
Tim:
What are you thinking about all this, Derrick? When all this is going on, what's going through your mind? Not the crash, the ramp up into it, we'll get to that.
Derrick:
Oh, the ramp up into the business?
Tim:
Yeah.
Derrick:
Oh, I was all for it. I was coming from a little bit different perspective of Josh. Josh has the plant biology background under his belt where I had more of the medical side. I came through a ... My process of being a personal trainer and a crossfit coach and then going to physical therapy assistance school, getting a degree in exercise science, business management, like so that's where I came from is seeing people who were utilizing either THC or CBD as a health and wellness mechanism and then I got to see the dichotomy of people using opiates and I don't think I have to go into the opiate crisis that Utah is going through. So, I saw what those were doing for people and then right around that same time, Josh comes with this idea and it was just kind of an easy transition for me.
Tim:
So, 15 locations and you get one-
Josh:
We finally got one. I mean we have to be completely transparent from the get-go. You can't like ... You can't say we plan on growing plants and then let them find out it's cannabis later. So, we finally found a landlord that was willing to work with us, locked in the lease, supplied for the licenses, got the licenses and then started the process of getting our business license and our first crop went in end of 2019 and we were like, let's do this, it's great. The only thing that can shut us down is if the world were to stop.
Derrick:
And that'll never happen, right?
Chris:
Right, I mean that'll never-
Derrick:
Something happened in 2020 that shut the world down.
Josh:
2020 hits and ...
Tim:
Yeah, this is 2019.
Chris:
Now, did you end up getting a place here in Salt Lake? I mean obviously, I don't need to know the exact location but what area are you in kind of because we've chatted with people in Logan, Sandy, I was just kind of curious about where you were at.
Derrick:
Yeah, we're in South Salt Lake, a little-
Chris:
Okay, okay.
Derrick:
... about 1800 square foot warehouse.
Chris:
Okay, indoor grow?
Tim:
Everything's indoor?
Josh:
Everything's indoor.
Tim:
Why do you want to do indoor? Was that a choice?
Josh:
Yeah, I prefer indoor hydroponic or aeroponic just because of the level of control that you have over the plants. It's a lot harder to do and you have a much, much smaller window than using soil but you have a much higher level of control in like your nutrient uptake and your water uptake and your lights and everything.
Tim:
Right, you can control the spectrum of light, the timing of the light. We've been to some of the medical grows and yeah, I mean they control everything.
Josh:
Yeah, I basically used everything that I had learned growing THC and just translated it directly over to help.
Tim:
Where'd you learn that?
Josh:
I spent a year up in Oregon supervising my own grow and making every mistake you can make, like powdery mildew, mites, fungus, gnats, everything, like too much humidity, but I needed that in order to learn what to do and what not to do.
Chris:
We were just talking about Oregon before you guys-
Tim:
I know, we were.
Chris:
... the prices of some marijuana up there.
Tim:
Yeah, the prices of product.
Chris:
An ounce for like what $60 for an ounce?
Tim:
Yeah, grand opening prices, $60 for an ounce, $60 for a top shelf half ounce, I mean it seemed like-
Chris:
Wouldn't you like those prices to be here?
Tim:
Yeah, right.
Derrick:
That'd be great.
Tim:
Yeah, I mean alternatively, though, you don't, right? Because you're in business and like Bob Waters said, "Revenue is fuel."
Chris:
True.
Josh:
True, there is a way though to be profitable at those prices still.
Tim:
Yeah.
Josh:
And I mean the ... I don't know the total acreage that they said that's needed to supply the entire United States with THC flower is like less than a 100 acres or something.
Tim:
Yeah, just because-
Chris:
Really?
Tim:
Because the plants grow so well. They don't require as much water. Because you have an indoor grow, all of your products then, or all of your grow is really based on not biomass per se, it's on flower?
Josh:
Yeah, mm-hmm (affirmative).
Tim:
And what you can extract from the flower?
Josh:
Well, we're not doing any kind of extraction. We actually ... We hit up Mountain Valley Botanicals. I call them up and I said, "I need to get some flower extracted." And he was like, "Okay, how many pounds are you working with?" And I was like, "10." And he was like, "Oh yeah, our minimum size is like 1000 pounds." I'm like okay, nevermind.
Derrick:
Okay, let’s go.
Tim:
So, really, you focused in ... I'm looking in on your website and you focused then a lot on raw flower.
Josh:
Yup.
Derrick:
Mm-hmm (affirmative).
Tim:
But you weren't able to sell raw flower up until now? How does that work in Utah?
Josh:
Well, so we started Uinta Cannabis to sell flower and flower products to customers and then UDAF axed that with the registration law, basically saying products need to be registered in the state of Utah but we will not register any flower or food additive products, which killed our business plan. And so we went to the drawing board thinking what are we going to do? Is this is end? We've been in business for less than a year and-
Tim:
You've sunk all your money and everybody you're close to's money.
Josh:
Yeah.
Tim:
Into this thing.
Josh:
Yeah. We had tried approaching the pharmacies but before the law changes, there was already enough red tape that it was a little bit cost prohibitive and now, since the law changes, it's just like almost impossible to get it into the pharmacies and so we thought what do we do? And we came up with the idea of starting up a marketplace, a true marketplace for farms in Utah to get their flower and flower products out to the rest of the nation. Well, we couldn't start a company in Utah, so we started a company in Nevada, completely 100% separate from Uinta Cannabis to act as a true marketplace and from the beginning, we're the only farm that's listed on it and we were thinking maybe summer of 2021, one, maybe two farms will approach us and say hey, we're interested in getting on your marketplace and what can we do.
Josh:
Within the first week of going live mid-December, we had three farms reach out to us saying hey, we need to meet.
Tim:
Three farms from where? From Utah?
Josh:
From Utah. We only carry products from Utah farms.
Derrick:
Yeah, but…
Josh:
Specialize in things grown in Utah.
Tim:
And you realized…
Chris:
This is for utahhempgrowers.com, right?
Josh:
Correct.
Tim:
Right, so this is how Utah Hemp Growers got started?
Josh:
Yup.
Tim:
That's a Nevada company-
Josh:
Yes.
Tim:
That is a marketplace for, basically, Utah hemp products to be sold around the nation but almost like a co-op?
Josh:
Not really. I mean there's set boundaries established.
Tim:
Or do they just come and say, hey, look, we want to sell our products. We want you to help us network get these accounts set up and find places where we can sell our stuff?
Josh:
Well, we just open it up to the nationwide marketplace and-
Chris:
Everybody can buy it.
Tim:
Even Utah.
Josh:
Everybody, exactly-
Chris:
Even Utah people can buy it-
Tim:
Because you're out of Nevada, so you can buy it back to use?
Derrick:
Yeah, that was kind of our main focus is to be able to get flower here.
Josh:
And one of the biggest risks in the hemp market is because so much of it is online, you're having to take a risk as a customer of buying from a company that is brand new, that you've never heard of and that you've never met and so from a farmer's perspective, what's better than being able to sell what you've grown to your community and show-
Tim:
Well, of course, I mean that's the whole point. We talked last week about this to Margie up in Cash County.
Chris:
The Hemp Folk.
Tim:
Yeah, The Hemp Folk, where this ... People want to buy tomatoes from the local farmer-
Josh:
Yeah, exactly.
Tim:
And they're going to want to buy, eventually, right-
Chris:
Some local CBG.
Yeah, right?
Josh:
Keeps the money in the state too.
Tim:
That's right but you've had to go out of state to get it back in?
Josh:
Yes.
Tim:
A story we've heard three or four times now.
Chris:
I mean was that tough to set up? I mean, were there hoops that you had to jump through for that?
Josh:
It's been a minefield of regulation, just tiptoeing and finding out-
Tim:
Even though it's in Nevada? Even though-
Josh:
... how to do it right.
Tim:
... Nevada's ... I mean Nevada's full legal for everything, really. So there probably wasn't a lot of laws for Nevada that you had to jump through.
Josh:
Yeah, but well, the big sacrifice is we package and fulfill all of our shipments in Nevada and so there have been weeks where we will get one order and it's a $20 order and we wait a day, maybe two days to see if more will come in and then we just have to bite the bullet, drive out to Nevada, fulfill the order and get it shipped and drive back.
Chris:
So, you have to do everything in Nevada? You can't do it here in Utah?
Josh:
No.
Tim:
Because it has to be postmarked, that's the key, right? You can't hide.
Josh:
Yeah.
Tim:
Because the postmark. If that person was on UDAF and he made the order and it was postmarked here, you're done.
Josh:
Yeah.
Tim:
Okay, so-
Josh:
There's people doing it like that here but-
Chris:
Fun to learn about.
Josh:
We don't delve into that.
Chris:
People don't realize the obstacles that these guys are jumping through in the ... How much extra work they're doing for really little pay if you ask my opinion.
Tim:
I totally agree and I think also that every time we talk to another hemp grower, we talk to another person in the cannabis marketplace that is not ... Specifically not in the medical side, the hoops that you have to jump through, you have to find the hoop, you have to find a way to jump through the hoop. No one is there to help you. The regulations are not clear. Every state is different whereas with the medical program, it does seem like those rules are set. It costs a lot of money to get in. You're going to have a big infrastructure to do those things that you have to comply, right? To follow those compliance rules? And even though it seems it's hard to get into the medical side, it does seem more straight forward.
Josh:
Yeah, mm-hmm (affirmative).
Tim:
Would you agree with that?
Josh:
Oh yeah. Mm-hmm (affirmative), yup. The rules for the Utah hemp industry are unclear. They're pretty undefined.
Tim:
And they that way, do you think, nationwide or is Utah unique there because I've also heard that Utah's hemp laws are some of the best or most progressive or the marketplace is growing better. Is that just marketing?
Josh:
I would say it's just marketing. I mean most of the country's going off of USDA laws and with this recent change allowing flower on the shelves, it may look like a step forward but the current writing with 0.3% total THC post harvest means that your Delta-9 levels need to be 0.03 because you have to account for the other cannabinoids to stay under that 0.3.
Tim:
Okay, so let's talk about the new law changes a little bit and let's dig into this. Okay, we're pretty clear on 0.3% or less of THC in any flower. So the law change ... Explain what the law changed in Utah with flower ... With hemp flower or CBD flower.
Josh:
So, it allowed for hemp flower and hemp flower products to be sold in brick and mortar, in-person, but it changed the wording to 0.3% total THC with a post harvest COA that has to be full-panel as well and then you have your-
Tim:
Uh-huh, so it includes Delta-10, Delta-9, Delta-8-
Josh:
Everything.
Tim:
All of the Deltas-
Josh:
All of the cannabinoids.
Derrick:
All of them.
Josh:
And that needs to be…
Derrick:
0.3 or lower.
Tim:
Okay.
Josh:
And this is after harvest when the plant is more likely to spike in its cannabinoid levels-
Chris:
Wow.
Josh:
So, USDA rules are 0.3 Delta-9 pre-harvest, before the plant has a chance to spike and you're only measuring one cannabinoid. Utah is all the cannabinoids post harvest and that number needs to be below 0.3.
Tim:
All the tetrahydrocannabinol post harvest, not the CBD, CBG, CBN, all the tetrahydrocannabinol-
Josh:
Yes, mm-hmm (affirmative).
Tim:
Which is a lot of Deltas, right?
Josh:
Yeah.
Tim:
Now, this is specific because in other states, they've had Delta-8, this came up. I think ... Tell me if I'm wrong, Delta-8 has been manipulated in other markets to sell something that will kind of get you high?
Josh:
Yeah, and for Utah Hemp Growers, we believe that that's an imperfect practice. So we have it stated on our website, we will not carry any of that sprayed flower because that Delta-8 extract, it can be extracted or it can be synthesized. You have no idea where it's coming from and you don't know, unless you have a reliable, full-panel COA, you don't know the amount of solvents that are still in that and so what we're seeing is there's a lot of people that are ... I mean just straight with a paint sprayer, they just spray down the buds with this Delta-8 solution and then try and move it out the door to give you kind of an extra kick. It's kind of weird. It seems like the new spice hype.
Tim:
Sorry, I had a patient recently that talked about the difference between Delta-8 and Delta-9 from an experience standpoint because there's not a lot of research in the uptake of Delta-8 in the body. It does seem to be a peripheral uptake, not a brain uptake as much and he described ... He smoked a half a gram of Delta-8 concentrate and he just described it as this almost tingly, numbing type feeling throughout his limbs.
Josh:
Oh wow.
Tim:
A much more peripheral experience where he didn't have that psycho activity but it was still ... It still had a significant effect, right?
Josh:
Yeah.
Tim:
And that Delta-8 seemed to be like the reason they changed the rules and the language in the law for the hemp side.
Josh:
Yeah, it's a big factor in why they're doing it.
Tim:
But it makes it really hard for you guys to take total THC and keep it under 0.3.
Josh:
Yeah, nearly impossible.
Tim:
Really?
Josh:
Yeah.
Tim:
What happens if your flower's 0.35 or beyond the ... There's some sort of buffer.
Josh:
Yeah, there's the 15% buffer. So you can go to 0.35 and still be able to-
Tim:
Still be technically legal?
Josh:
... put it on the market.
Tim:
But what happens if it's 0.4?
Josh:
0.4, you're allowed to remediate it into oil or destroy it without penalty and if you go above 1%, then they just notify law enforcement.
Chris:
And then law enforcement comes and arrests you?
Josh:
Yeah.
Tim:
Then the black suburbans show up, oh my god.
Chris:
Even though you didn't try to. I mean you grew hemp but then it ... I mean what are the chances of it being too high?
Tim:
Yeah, how often do you get a hot ... What do you call it? A hot crop?
Josh:
A hot crop. Going over 1% is pretty hard.
Chris:
Okay, okay. That's why I was like, I wonder how hard is that? That might be kind of scary.
Josh:
Yeah, so I mean I can see why they wrote that but it is pretty intimidating.
Chris:
Yeah, noted, noted.
Tim:
I mean is there a way for you guys to test it before they come and test it?
Derrick:
So, we have a pre-harvest test that we pass. So that's come and done ... Performed by the state and then we have a certain window and then we have to do a post-harvest test.
Chris:
Well, I'm just wondering like that you guys can keep an eye on to make sure you're not getting too hot?
Josh:
Yeah, I mean and growing the same strain over and over again-
Chris:
You kind of figure that out?
Josh:
... we know where it's going to be and when it's going to be and when it's going to ... If and when it won't be compliant and so, there was one strain that we grew first that wasn't compliant and we got rid of it because it just ... It didn't ... It wasn't even compliant when they came in pre-harvest.
Chris:
Oh right, so you're like this is not going to work out, it's just too hard. There's plenty of other strains. How many strains do you get to choose from before you grow? Are there plenty of options?
Josh:
Oh, there're tons of options.
Derrick:
Tons, yeah.
Tim:
Really?
Josh:
It doesn't mean that it's going to be quality in the end but there're tons of options out there, yeah.
Tim:
And do you buy seeds or clones?
Josh:
Well, we start with seed and then if it turns out to be a phenotype that we like, then we'll go off of clone off of just that one phenotype, just for control.
Derrick:
Yeah, like we've had three strains that we just pushed out that we didn't like how any of them turned out as far as weight and we haven't had a chance to partake upon them yet but just the way that they're growing and stuff, they're just not really probably what we're going to continue with. So, we're not stuck on any strains but we do have like our flagship, our Blue Mint. It's a cross-strain of Charlotte's Web and Harle Tsu that's just phenomenal and you can't get it anywhere else.
Tim:
Is the cannabinoid content ... Like do you look for mixes of certain type of cannabinoids? Like the Blue Mint, describe that. Like what's the cannabinoid content in something like that?
Josh:
Our CBD in that runs anywhere between like 13 and 15% but we're not chasing any specific cannabinoid and we're not chasing a terpene profile. We just try the flower. We give it out for samples for professional reviews and get feedback and there are some strains out there that we've sampled that are 25%, 28% CBD that just don't cut it. So we're not chasing any kind of specific profile-
Tim:
You're chasing the experience?
Josh:
Yeah, does it have a good experience? Does it have good effects-
Derrick:
Yeah, because it's medicine.
Josh:
Good smell? Good look?
Tim:
Yeah, and you're hitting on a point here where the entourage effect of an interesting profile based on the person that consumes it, the way it's consumed and that sort of thing can change, even regardless of the content. I think there is too much put on, for example, the percentage of THC in a flower, right?
Josh:
Correct.
Tim:
And we talk about this all the time.
Chris:
Every episode it seems like, right?
Tim:
Yeah, how the THC content, the percentage doesn't matter, right? There's been good studies that compare 15% THC to 25% and the reporting is that you just get just as high, right?
Josh:
Mm-hmm (affirmative).
Tim:
Or the experience is just as psychoactive. So, I like that approach, that's pretty cool.
Derrick:
Yeah, the education needs to be ... To just catch up and be spread more and more and I think that it'll catch on over the next few years, hopefully, that people stop chasing individual cannabinoids. Just because it's 33% THC doesn't mean that it's the flower that's right for you.
Chris:
Yeah.
Tim:
Yeah, interesting. So now, how, with the law change though and you've got good product and it meets all the requirements, now can I go to your shop and buy it?
Josh:
Our website, because we don't have any physical locations?
Tim:
Okay.
Chris:
Well, can we go on your website and get it shipped directly from-
Tim:
Yeah, can now ...
Josh:
Yep, directly to your door.
Chris:
So, you don't have to go to Nevada and ship it to me now?
Josh:
Well, no, now ... Well, we still have to drive to Nevada and fulfill it but we can have it shipped right to your door.
Tim:
Okay, but how did the law change to allow smokable flower to be sold in Utah?
Josh:
If it's being sold in Utah, if the transaction is taking place in Utah, then that product must be 0.3% total THC or less, have a full-panel lab post-harvest and be registered with the state, which I think is like $350 per product.
Tim:
And that's every time you harvest? Probably.
Josh:
Yes, you must also, if you are going to fulfill that yourself, you have to have your cultivation license and a processing license now.
Tim:
For hemp?
Josh:
For hemp, for hemp.
Tim:
But you can still drive to Nevada and ship it back into Utah without following that part?
Josh:
Well, because we're a Nevada company operating under Nevada laws under USDA laws-
Tim:
Oh my lordy.
Chris:
So, even with this new law, it doesn't even matter.
Tim:
So, do you feel like the law is a benefit or is it a step in the right direction or does it just create a different set of issues?
Josh:
it's a different set of issues because it's going to open up the floodgates for low grade flower on Utah shelves-
Derrick:
People are going to-
Josh:
Because it has to stay under that percentage.
Derrick:
Yeah, people are going to get their first hemp experience buying let's say a pre-roll in a store and it's going to be a less than ideal experience.
Chris:
Because the company that makes that pre-roll or sells that flower is probably going to be a company that just grows in bulk and is there to make the profits and they just want to sell a product on the shelf, but they have enough money to jump through those new hoops?
Josh:
And staying compliant with that 0.3 total THC, that flower is going to have very, very low levels of all cannabinoids.
Tim:
And again, we have got to get to a point where we can have a range of zero THC all the way up to 30-whatever percent there is now and find ways to allow people to make these choices with their, in my opinion, medical provider, who can help make these choices on hey, you know what? You don't want to get stoned out of your mind but you need something that's like 1% or 2% THC, right? Because there's none of that on the market.
Josh:
Yeah, mm-hmm (affirmative).
Tim:
Right, that doesn't exist.
Josh:
It's either high CBD or high THC batch.
Tim:
It's 12-plus, 12 is way low THC or it's 0.3% and less.
Derrick:
Mm-hmm (affirmative), yeah, we're getting really good feedback though on people that are mixing on a one-to-one ratio.
Tim:
Okay, so talk about that with regard to your products, like what's the process of using these products and how best do we use them? Teach me. Teach me how to incorporate hemp flower, non-psychoactive essentially of cannabis flower into my regimen.
Derrick:
Well, I should say, it is psychoactive. It's non-intoxicating.
Tim:
Got it. Okay, you're of the school that, okay, when I say well, CBD is not psychoactive and you're like well, actually, if you go to the definition of psychoactivity, then yes, it is because it's calming-
Derrick:
People will feel an effect-
Tim:
Right, you can feel an effect.
Derrick:
... but you will not be intoxicated to where you're couch locked or-
Tim:
Okay, yeah, totally fair.
Josh:
Yeah, it takes off like that top heaviness.
Tim:
Cannabis/marijuana, marijuana/cannabis.
Derrick:
Yeah, right.
Josh:
You can use it during the day for some strains ... Well, for a lot of hemp strains to help with anxiety, inflammation, energy. Mixing it, people like to say that CBD nullifies THC. It does not nullify it. It works alongside it to help balance it out to where you're not getting that spiral effect from ingesting too much THC and now you need to lay down because the world is spinning around you. It helps to balance that out to where you can have a nice psychoactive effect from the THC without going down that spiral.
Chris:
You're building your own 3% product or 5% product essentially.
Derrick:
Correct, yeah.
Chris:
Right?
Derrick:
Mm-hmm (affirmative).
Chris:
From a physical standpoint, when you're talking about training and you had talked about your coaching, Derrick, before, I mean do you see that more and more people in your old world, the crossfit world, the people who are really into their health are moving this direction?
Derrick:
Yeah, absolutely. People are sick of all the fillers in all the medicine. They're sick of balms not really working whereas we have a salve that's actually like healing people. They're not having to kind of rely on it for a daily thing, they're using it for like a week and their injury is fixed.
Josh:
Yeah, we're careful not to make any medical claims and so all of this feedback is just ... It's coming unsolicited from customers that just send back feedback saying, "This helped me." We've had feedback from people with epilepsy saying, "This is changing my quality of life. This flower is changing my quality of life," and we're not putting out, "Oh, this will fix your epilepsy." We're not saying that. We just say, "Here's a product that has passed out standards for quality and we're putting it out there because of its medicinal benefits. Use it as you see fit." And then we get the feedback of people saying this is changing my life for the better.
Tim:
Oh, that's cool. Do you want to get into the medical side?
Josh:
Eventually, yeah, that'd be great.
Chris:
When a license opens up, I guess, huh?
Josh:
And we have the …
Chris:
But at least you'll have the experience now, right? And you'll kind of already have your foot in the door.
Josh:
Correct.
Derrick:
Oh yeah.
Tim:
Yeah, and how many square feet is your grow?
Josh:
We have a total of about 1750 square feet and we're using a third of it but we're working on filling up the rest of it. So we're really small.
Tim:
Yeah, yeah but as far as that goes, though, I mean it gives you really good opportunity to learn, grow, get established and then I mean, heck, there will be more-
Chris:
Oh, there'll be more. There'll be more.
Tim:
... medical here eventually. They'll need more. They'll need more different types of people and Utah's interesting. When you look at like beer sales or beer ... Like the breweries, for a longtime, it didn't seem like Utah was a good place to buy beer-
Chris:
It's one of the best now.
Tim:
But it's one of the best now.
Chris:
In my opinion.
Josh:
Yeah.
Tim:
Yeah, I mean we win all kinds of awards and even the low alcohol content of the beer almost made people work harder to make better beer-
Derrick:
Yeah.
Tim:
... and that craft product could translate into cannabis-
Derrick:
Exactly.
Tim:
... in Utah. We seem to be that type of group.
Chris:
It'll be craft cannabis here, right?
Tim:
Right? And have some craft cannabis groups with small grows and-
Josh:
There's always going to be a market for that small craft cannabis grow.
Chris:
Yeah. So, a couple of weeks ago we were talking to Margie, from The Hemp Folk, and she was talking about some interesting stories of mailing hemp. Have you guys run into any like interesting situations as far as hemp not getting to people or anything like ... Yeah, she was telling us like-
Tim:
Oh my gosh.
Chris:
... she lost like $25,000 from one-
Derrick:
Oh wow.
Josh:
Yeah, well-
Chris:
... The post office just kept opening up her packages.
Derrick:
I wonder if she had like writing like her business name on there, yeah.
Chris:
The smell. I guess it was the smell.
Derrick:
Well, we haven't had any issues with smell. The bags that we use are reliable and we're actually phasing them out to get the child-proof bags. It'll be more expensive but we're staying compliant with how Utah has written the laws, so we changed up our labeling to be compliant and now we're changing up the packages, even though I would say maybe 5% of our orders actually go to Utah. The rest of them go to the rest of the states but we've had-
Chris:
Oh, interesting.
Derrick:
... Yeah, we've had no issues with the packaging. I actually ... When I sent out my first package, I had written Utah Hemp Growers on the return address-
Tim:
And you're like, that's a bad thing.
Derrick:
Well, the lady at the post office was like, "You should probably not do that."
Tim:
Yeah.
Derrick:
Like just giving you some advice and so it really is just avoiding those things that say like CBD, hemp, cannabis, anything on the packaging that advertises it because then all it takes is one curious set of eyes to pry open your package and now it's delayed. It never arrives. You lose your money.
Chris:
Yeah, you can put like ... I'm trying to think of something to put. BYU or something like that.
Tim:
It's the same thing with us, right? At Utah Therapeutic Health Center, our logo is the state with a cannabis leaf in it and we have a logo without the leaf because there are documents that we need to send that don't ... They don't need that type of scrutiny, right? And it is a part of this business.
Chris:
It's sad though that it has to be that way.
Tim:
Yeah, I think that it's changing a little bit certainly you don't want to go to the bank with that logo, right? You've got to have a name that the bank ... The bank knows what you do but the bank needs to check their boxes and dot their Is and cross their Ts and they need their applications to flow through.
Chris:
But do you remember ... I remember like back in the 90s, it seemed like it was the 90s, that like friends would wear like pot shirts and you'd be like, "Oh my gosh, you're just asking to get tarred."
Josh:
Yeah, for sure.
Chris:
Now, people wear it and it's like, it's okay.
Tim:
It is true. Now, this morning-
Chris:
So, it just goes to show-
Tim:
... We had this conversation at my house because we have some T-shirts that are healthcare-
Chris:
That have pot leaves on them?
Tim:
... to buzz about and they have the THC molecule on them and a couple of bees and they're super cool T-shirts, I really like them. And then on the back, it's classy on the front and then on the back, it says, utahmarijuana.org. And my son, who's in sixth grade, he comes to me and he's like, "Hey, it's St. Patrick's Day, I don't have anything green, what do you think, Dad?" And he laughs. He just chuckles. He's like yeah, they'd kick me out.
Chris:
No, but I mean there was a time when you-
Tim:
You can only go so far.
Derrick:
Yeah.
Chris:
... couldn't wear it. You'd be targeted.
Tim:
Oh yeah. Well, the Utah in the Weeds sweatshirts, right? We wore those around all the time.
Chris:
Yeah, and you couldn't wear-
Tim:
No way.
Chris:
... Like 20-30 years ago, you couldn't do that.
Tim:
Oh yeah, there's no way.
Chris:
But so things are changing.
Derrick:
The one kid with the weed hoodie in high school and everyone looks at him like, we know.
Tim:
Yeah, like oh, we know. Yup.
Chris:
Yeah, because it's like oh yeah, you're just a supporter.
Tim:
Right, oh yeah, sure you're an advocate.
Josh:
That was actually my first experience with cannabis is back in high school. I actually tried growing it.
Tim:
You did?
Josh:
Yeah.
Chris:
Did it fail or did you succeed?
Josh:
Oh, I thought I was like on top of the world and I was acting so stealthy and I had three little plants in solo cups under my computer desk and of course, I got caught like almost immediately-
Chris:
By your parents?
Josh:
By my parents.
Chris:
Oh, okay, okay.
Josh:
Who called down to the principal's office and the school officer's sitting there with the vice principal and this actually started my path into cannabis because she asked me, she was like, "Why were you growing?" And I told her, "My friends smoke and so I figured I would just grow it and they're spending all this money on it, that way they don't have to spend money on it and I'll be the favorite friend of the group." And she looked at me and she was like, "Do you want to kill your friends?"
Tim:
Oh my gosh.
Josh:
And I was shocked because I didn't know anything about it and so I just looked at her and I was like, "Of course not. What did I do?" And so I caught a suspension for that and when I got back, I went to the school library and checked out every single book on cannabis that I could find.
Tim:
Oh wow.
Josh:
And just started reading.
Chris:
Were there a lot?
Josh:
Yeah.
Chris:
Oh wow.
Josh:
People were like ... Oh well, like my classmates were like, "Can you be reading that?" And I'm like, "I assume. I checked it out."
Chris:
I checked it out from the library.
Josh:
Yeah, and I just started reading on the history and everything and was like, she lied to me.
Tim:
Then you go into the military, both of you have military backgrounds, yeah?
Josh:
Mm-hmm (affirmative), yup.
Tim:
You're air force, Josh?
Josh:
Yes.
Tim:
Derrick?
Derrick:
Navy. I was almost seven years intelligence.
Tim:
Wow.
Derrick:
I was a communicator, so I did satellite communications, radio comms, point-to-point, network security, things of that nature.
Tim:
That's pretty cool. Have you guys seen the new Army ad, the commercial where it looks like a game and they've got the communicator, they've got the warrior, right?
Derrick:
Oh, I've seen that, yeah.
Tim:
The fighter. They've got the replenisher and the chef slices something like the Kung Fu Panda game and then I mean it's pretty cool but they've definitely changed their approach of recruiting to a younger generation.
Derrick:
Yeah, I'm sure the military [crosstalk 00:38:49] sweeping water in a rainstorm.
Josh:
Oh yeah.
Derrick:
Or sweeping water on a ship out in the middle of the ocean.
Chris:
Did you have to do that?
Derrick:
Oh yeah.
Chris:
Wow.
Derrick:
Oh yeah, I did two deployments on a ship and then one actually where I was boots on ground in Baghdad and so I go to see the silliness of a shipboard deployment and then what it’s like being attached to detainee operations at a joint taskforce.
Tim:
Hmm.
Chris:
Wow.
Tim:
Interesting. And in the military, did you have any exposure to cannabis in the military?
Derrick:
No, just keeping up with the news and everything. Like seeing the news in 2012 with Colorado legalizing and being like oh, great, I can do nothing about that.
Chris:
I can watch, yeah. The military kind of frowns on cannabis, right?
Josh:
Yeah, I was actually in ... I was stationed in Colorado Springs right around the time when that all went legalized, so ...
Chris:
But you can't partake in Colorado Springs even though it's legal?
Josh:
No, no sir.
Chris:
Because you're federal.
Josh:
Correct, yeah.
Tim:
Actively engaged in like ... Receiving funds from the federal government other than being a veteran. If you're a veteran, you can't lose your benefits for using state-regulated medical cannabis but if you're active duty, work for the FBI, work for anybody, you can't touch it. In fact, I mean we have friends in the state department that they don't even follow us on Facebook or ... And they're close friends. They just can't have that sort of stuff coming up on their feed and I mean she doesn't even email me.
Chris:
Even hemp and CBD, you can't even ... Could you use hemp or CBD products in the military?
Josh:
Nope.
Derrick:
No.
Chris:
Today, could they?
Josh:
Anything cannabis.
Derrick:
No, yeah.
Chris:
Like even just go to the gas station and get some CBD tincture, they can't even use that?
Derrick:
Absolutely not.
Josh:
No.
Tim:
Now, I've had guys that work up on base and are even scared of a zero THC/CBD product just because they're ... And they just don't want to take any chances.
Derrick:
Yeah, yeah, there's zero tolerance.
Tim:
Now, so even last night, though, I was reading some studies on PTSD and cannabis treatment and the Canadian government almost takes the opposite approach. So the only people-
Chris:
Here, get high.
Derrick:
They're so lucky.
Tim:
... in Canada that get free federally covered cannabis as medicine, that's covered under their national healthcare, are military veterans. Move up there and if you're a veteran of the Canadian military, you're covered. You can go into the dispensary and they will buy your cannabis for you.
Josh:
Yeah, and they can grow beards, which is awesome.
Tim:
And they can grow beards.
Derrick:
That's great.
Tim:
Yeah, it's just such a different approach.
Josh:
Yeah.
Tim:
And right across the border, right?
Derrick:
Yeah, and active duty, as long as it's not directly interfering with your work, you can consume all the alcohol you want.
Chris:
Oh, really. That'll change here in the US. I think maybe the US will eventually get a little more onboard with their military.
Josh:
Yeah, I would think so.
Chris:
10 years, 20 years maybe.
Josh:
I don't know, however long it takes. I mean there're the alternatives. This is the thing that I was researching, is really the alternatives between cannabis and other medications and that's really where it comes down to is the companies that make benzos and opioids, they don't want us to stop prescribing those and so they don't want to do any research on comparative ... Does CBD or does hemp flower, smoking hemp flower help you reduce other prescription use? That's what we need to start. That's the research that's not been done yet.
Derrick:
I think they've done it in Colorado, several studies, that have shown a year by year decrease in prescription opioid use since legalization.
Josh:
Yup, mm-hmm (affirmative). There is. There is definitely an association with or a correlation with decreased prescribing of opioids and benzos too.
Tim:
So, you have the balm, so you have some type of products ... some products are processed, not a lot of products?
Derrick:
We took just a shot with our balm, just let's make a tiny little batch and see what happens and so the feedback has been great. So the next step is we get our processing license. We start adding more lights and we just keep going.
Tim:
Okay, so you've got to grow more, you've got to process. So you got to move to the next step?
Derrick:
Yup. Yeah, proof of concept is kind of what we were going for instead of just rushing into it and having all kinds of product or debt that we can't fulfill. So we have our proof of concept down, we have kind of our flagship strain, so we're kind of ready to rock and roll.
Chris:
Is it just the two of you? Do you have like employees, like other people trimming or anything or just the two of you?
Josh:
Nope, it's just the two of us running both companies.
Chris:
Okay, that's cool and is the marketplace growing?
Josh:
Yes. The marketplace for high quality hemp flower. Now, there's a lot of average and low quality flower out there since everyone jumped on it, grew 10, 20, 50, 100 acres and now they're sitting on it and they don't know what to do with it and so finding the high quality flower is a challenge but I mean we're taking it on.
Tim:
How do you guys market?
Josh:
That's tricky.
Derrick:
Like this, word of mouth. Yeah, just getting our name out there.
Josh:
We have no SEO, so we can't do any kind of online advertising. We have to be careful with any kind of ads that we do put out. We were lucky enough to get a full page ad in the Salt Baked City Magazine, their first one.
Tim:
That's right, yeah.
Derrick:
Page six or so.
Tim:
That's right, you guys were right by us.
Josh:
Yup.
Derrick:
Yes, sir.
Josh:
And yeah, there's a promo code in there if people want to get their hands on it and check that out. We want people to go out and get it.
Chris:
Okay.
Tim:
Yeah.
Josh:
And check it out.
Chris:
So, use that promo code there in Salt Baked City.
Derrick:
15% off little nugget in there for anyone that wants to go and look.
Tim:
Yeah, and you can pick up those magazines at any of the pharmacies. You can pick them up at any of my locations, my clinic locations, Utah Therapeutic Health Center. Yeah, they're free. It's a free magazine. Salt Baked City, our ad, Utah in the Weeds, is in there. You guys have stuff in there. They focused on a lot of really cool-
Chris:
Beautiful, beautiful publication.
Tim:
Yeah, it's a beautiful layout. And it describes a lot of the process of the over the course of the year and the people who are really involved in that.
Josh:
Yeah, I'm looking forward to more.
Derrick:
Yeah, the guy who published it is an incredible guy.
Chris:
Oh, yeah.
Derrick:
Yeah, he really wants to progress the community and we're happy to be at his side, so it's really great.
Chris:
Oh cool. Sure. What would you tell somebody ... Like let's say I've asked this of a few people that come on the podcast, somebody's questioning whether they should try some sort of cannabis for something they're dealing with and they're a little skeptical of trying it. Is there any advice or suggestions or anything you would tell them if they're listening right now?
Josh:
I mean if it's THC-
Chris:
They're maybe a little worried, I don't know. Yeah, let's say THC.
Josh:
THC, well, even CBD, we're going to be offering like a flower sample pack. So you can get just small amounts of each and try it out-
Chris:
Try it out, yeah.
Josh:
Try one and give yourself ample time to feel the effects and for the effects to dissipate before you try something else. Don't just try one strain, try another strain, try another strain because then it kind of jumbles all together and you won't get an accurate representation of how that strain is helping you or if it's not. But start with a small amount and then when you find something that works, use it and don't chase a cannabinoid. Don't try and say, I just need the highest THC, I need the highest CBD, I need the highest of this one terpene because you don't know what strain is going to work and what strain isn't until you try it.
Chris:
Exactly.
Tim:
This is just good advice like for people who don't want to get high but they want to feel what cannabis feels like and they want to use it as medicine potentially, hemp flower is a good place to start.
Josh:
Yeah, mm-hmm (affirmative).
Tim:
The get into the experience, get a little dry herb vaporizer, grind some up, vaporize some hemp flower, see what it feels like. It's legal, completely legal, you don't have to have a medical card for it and it is a safe product to try.
Derrick:
Mm-hmm (affirmative). Yeah, and the standards that we go by, I mean, legally, what's required is for us to verify some kind of state compliance and that's it and we don't even have to post it. So, we take it upon ourselves to post all of our state compliance tests from all the farms that we work with and then post all of the full panel tests that we get so that a customer can see exactly where it was grown, what's in it, whether it's terpenes, a cannabinoid profile, the heavy metals, the pesticides, the insecticides, the moisture content, everything. They can see everything and they know exactly where it's sourced. So we're trying to provide a consistent, reliable marketplace for customers to buy from.
Tim:
Well, that's more than you can say about all the vegetables that we buy.
Chris:
Give the web addresses and how people can connect with the both of you or whatnot, I guess.
Josh:
Yeah, we're on Instagram and Facebook. Our IG is both uinta, without the H, uintacannabis and our other site is utahhempgrowers, all one word.
Chris:
And that's on Instagram too, I think?
Josh:
That's on Instagram. Yeah, both of those are Instagram and then we have a Utah Hemp Growers on Facebook.
Chris:
Very cool.
Tim:
Cool.
Chris:
So people, go connect, take advantage of that coupon. It's in Salt Baked City. Try some of the hemp from your website and say, hey, you know what? I heard you on Utah in the Weeds, right?
Josh:
Oh, absolutely.
Tim:
That's right. Yeah, cool. It was really nice to meet you guys. Thanks for coming down.
Chris:
Yeah, really great. Anything more you want to add? Anything more you want to talk about before we wrap this episode up? While the mics are still on?
Josh:
I mean we got ... For Uinta Cannabis, we have some new strains in the works and we just brought on our sixth farm that we're working with, so now we have ... Let me just name off the farms here. We have our farm, Uinta Cannabis. We have Carter Kids Construction, Hemp Ventures Utah, Honeycomb Hemp, Puff Hemp and I'm missing one.
Chris:
I'll tell you what, if you guys remember it, email us, we'll put it in the intro to the episode.
Josh:
Beautiful, beautiful.
Chris:
So, they'll be the first mentioned. So, when they get to the end, they'll be like oh, you didn't forget us.
Derrick:
Excellent, fantastic.
Josh:
Yeah, and then we're talking with other farms and I mean if they're growing good enough strains and it makes it through our standards, then we'll list it. So we're growing.
Chris:
Very cool.
Tim:
Cool.
Chris:
All right, guys.
Tim:
Congratulations, guys. Looking forward to seeing you grow.
Josh:
Lazy Roots, that's the one.
Chris:
Lazy Roots.
Tim:
Lazy Roots.
Derrick:
Lazy Roots with their pre-rolls. They're great.
Tim:
Cool.
Josh:
Yup, very cool.
Chris:
Well, thanks for listening to this episode. Make sure to subscribe on whatever podcast app you're listening to this in. Connect with Uinta Cannabis, Utah Hemp Growers, utahmarijuana.org/podcast is where people can listen to the podcast. Utahmarijuana.org is where they can connect with everything else, am I right, Tim?
Tim:
Yeah, they can connect with everything else we have and all right, everybody. Stay safe out there.
As you may or may not have heard, the 2021 Utah General Legislative Session was held this spring. Many amendments passed in multiple areas of the law in Utah, so rather than going blue in the face listing them all for you, let’s get to the good stuff: amendments to the Utah Medical Cannabis Act. What do patients need to know? What do providers need to know? Join me, if you will, and we’ll dive into some of the most significant changes made to Utah cannabis law and how they affect patients. (Check out this related episode of Utah in the Weeds with Rich Oborn, Director of the UDOH Center for Medical Cannabis.)
 When the Utah Medical Cannabis Act was written, it was stated that only fourteen Medical Cannabis pharmacy operating licenses would be awarded. All fourteen of those licenses were snatched up very quickly, but the rollout has been a slow burn. We still haven’t seen some of these pharmacies emerge over one year later. But, lucky for us — especially those of us in Southern Utah — every holder of one of the fourteen Medical Cannabis pharmacy licenses in the state will need to open by June 1, 2021. Our access to Medical Cannabis will almost double by summer!
When the Utah Medical Cannabis Act was written, it was stated that only fourteen Medical Cannabis pharmacy operating licenses would be awarded. All fourteen of those licenses were snatched up very quickly, but the rollout has been a slow burn. We still haven’t seen some of these pharmacies emerge over one year later. But, lucky for us — especially those of us in Southern Utah — every holder of one of the fourteen Medical Cannabis pharmacy licenses in the state will need to open by June 1, 2021. Our access to Medical Cannabis will almost double by summer!
But let’s get back to the session. First off, a bill passed through legislature that grants Utah one additional pharmacy license to issue, bringing the grand total to fifteen in the state. This pharmacy will be located in the rural area of either Daggett, Duchesne, Uintah, Sevier, Grand, San Juan, Emery, or Carbon County. UDOH doesn't have a deadline yet to award this license, but keep an eye out for it sometime in 2021. We suspect to see this license awarded to one of the existing players in the Utah Medical Cannabis space.
When 2020 came to a close, it left many of our Utah Medical Cannabis patients to the south and other rural areas up a creek without a paddle, so to speak. They were no longer legally allowed to possess cannabis purchased out-of-state, and the closest Utah Medical Cannabis pharmacy was miles away. Under previous law, out-of-state Medical Cannabis was deemed legal possession by active Medical Cannabis cardholders through December 31, 2020. A possession bill passed extends that deadline to June 30, 2021. This gives patients legal access to their medicine while the remaining Utah Medical Cannabis pharmacies get up and running.
In addition to this deadline extension for out-of-state purchases, a bill passed prohibiting patients to remove or alter the labels on their Medical Cannabis purchases. At utahmarijuana.org affiliated clinics, we have always suggested this to our patients as an extra precaution, but now it’s mandatory. Just think of the countless stories out there of legal Utah patients being pulled over with Utah Medical Cannabis in their cars being cited with possession. So, the more proof you have of legal possession, the better, right? You can’t always count on other people to know the laws. Many people in Utah still don’t know Medical Cannabis is even an option to them. This one just makes sense: keep your labels, folks.
Already rolling out in some of the pharmacies, more in-depth verification is coming for us in Utah. Every single Medical Cannabis transaction must now be reviewed by a Pharmacy Medical Provider before it’s dispensed. This could mean longer wait times and delayed pick-up or delivery orders while your friendly neighborhood pharmacist takes a peek at your dosage recommendations. There’s no doubt in my mind that this process rollout will be rocky at first, but think of it this way: you go to your local CVS or Wal-Mart with a prescription for 800mg Ibuprofen but ask for Percoset. If your pharmacist didn’t verify your actual prescription, you’d walk out with a controlled substance without a second look. That’s basically the thought process behind this law. It is a medical program, after all. We’ve got to treat this like medicine.
dispensed. This could mean longer wait times and delayed pick-up or delivery orders while your friendly neighborhood pharmacist takes a peek at your dosage recommendations. There’s no doubt in my mind that this process rollout will be rocky at first, but think of it this way: you go to your local CVS or Wal-Mart with a prescription for 800mg Ibuprofen but ask for Percoset. If your pharmacist didn’t verify your actual prescription, you’d walk out with a controlled substance without a second look. That’s basically the thought process behind this law. It is a medical program, after all. We’ve got to treat this like medicine.
A bill also passed this session stating that by Fall 2021, each Utah Medical Cannabis cardholder and their purchase history will be incorporated into Utah’s Controlled Substance Database. Likely the most highly debated amendment to the Utah Medical Cannabis Act, the pros and cons are clear. For example, many patients worry about discrimination or denial of treatment from medical providers who do not agree with cannabis use. With this new visibility, patients don’t get to choose who they share this information with as they do now. (Utahmarijuana.org pro-tip: it’s always best to be completely transparent with everyone on your healthcare team!)
That being said, there are some upsides to this inclusion in the CSD. This will allow for more access to research on Medical Cannabis use and treatment, which will only further the program not only here, but in other states as well. It’ll also promote honesty and provide a more effective and comprehensive patient-provider relationship. When it comes down to it, cannabis is an intoxicating substance at moderate-to-high doses and should be treated with caution by patients and providers.
 Buckle up for new EVS and card rules! I’m happy to announce that soon, our favorite necessary evil will get just a bit clearer. A bill passed to extend the timeframe of the first-issued Utah Medical Cannabis Card from ninety days to six months. That'll save patients (and providers) the headache of navigating the EVS application again so soon. Keep in mind that at Utah Therapeutic Health Center, we love to hear from our patients. Don’t be a stranger! If you need something in your first six months — application help, directions, program clarifications, anything! — please reach out to us. Our Patient Experience team is always happy to help or put you in touch with your QMP. You’re not alone in this.
Buckle up for new EVS and card rules! I’m happy to announce that soon, our favorite necessary evil will get just a bit clearer. A bill passed to extend the timeframe of the first-issued Utah Medical Cannabis Card from ninety days to six months. That'll save patients (and providers) the headache of navigating the EVS application again so soon. Keep in mind that at Utah Therapeutic Health Center, we love to hear from our patients. Don’t be a stranger! If you need something in your first six months — application help, directions, program clarifications, anything! — please reach out to us. Our Patient Experience team is always happy to help or put you in touch with your QMP. You’re not alone in this.
Next up. If you became a Utah Medical Cannabis patient in 2021, you’ve experienced the strange interim period of being able to use Medical Cannabis legally, but not being able to purchase it yet as you wait for your card to be sent to you. No longer! UDOH will soon roll out a Conditional Card available immediately to approved patients 21 years of age or older. For simplicity’s sake, think of Conditional Cards as fancy state-issued recommendation letters. Remember those? Providers can revoke this card at any time, and this will give patients access to the pharmacies while they wait for their Medical Card from the state. Look for Conditional Cards in the near future after necessary software modifications. We expect Conditional Cards to make an appearance on the scene in late 2021.
This session also introduced the LMP, or Limited Medical Provider. A Limited Medical Provider is defined as any MD, DO, podiatrist, APRN, or PA with a controlled substance license. (Oh yeah — a bill passed to add podiatrists to the list of approved providers that can be a QMP, too!) Contrary to a Qualified Medical Provider, an LMP doesn't need to register with the Utah Department of Health. In fact, they won't use EVS at all. However, they’re only authorized to recommend Medical Cannabis to fifteen patients. So, technically speaking, if your provider is willing, you could be one of the lucky fifteen they keep in-house. LMPs will roll out later in the year after necessary software modifications.
However, they’re only authorized to recommend Medical Cannabis to fifteen patients. So, technically speaking, if your provider is willing, you could be one of the lucky fifteen they keep in-house. LMPs will roll out later in the year after necessary software modifications.
Supportive of this amendment, Medical Cannabis education will appear in existing continuing education programs for providers with a controlled substance license. These providers already attend required courses every two years and these courses will soon include cannabis information. This will help support patients who choose to stay with their existing providers — cannabis experience or not — to receive well-rounded, comprehensive care.
In addition, physician assistant QMPs no longer require a supervising physician QMP (MD, DO, or podiatrist). Great news for PAs! Now you all can take a page from the Tim Pickett playbook with even more freedom and control over your practice. Score!
Finally, an EVS change. A bill passed giving QMPs the option to submit treatment and medication history about a patient to support their decision to restrict certain delivery methods or provide specific dosing guidelines into a patient record. This will be viewable by the PMP during the purchase verification process to ensure all recommendation guidelines have been met.
Phew! *wipes sweat from brow* Are you still with me? That was a lot to take in, wasn’t it? If we’ve learned anything about the Utah Medical Cannabis Program, it’s that nothing is set in stone. Things will change, then change again, then change back, and we’re all along for the ride. We here at utahmarijuana.org are here to keep you informed, safe, and legal. Keep an eye on our blog and FAQ page for the latest updates. For more about the program and these most recent updates, check out our founder’s podcast, Utah in the Weeds, where we interview Katie Barber, Medical Cannabis Program Specialist with UDOH, the man himself: Rich Oborn, Director of the UDOH Center for Medical Cannabis, and so many more. Comment below with your thoughts on these recent legislative changes — we’d love to hear what you think.
Episode 51 of Utah in the Weeds features a fascinating discussion with Derek Sherer, a medical cannabis patient with a history of opioid addiction. This particular episode is ideal for anyone concerned about cannabis being a gateway drug. From Sherer's perspective, it is an exit drug. [18:52]
Derek Sherer first started using marijuana recreationally at age 17. [03:19] In the years since, he has made a point of educating himself about its medical benefits. He puts that same effort into educating his children as well. [06:51]
His transition to Medical Cannabis began as a result of an opioid addiction some 14 years ago. [09:59] After breaking his hand three times and needing surgery, Sherer's doctors prescribed opioids. It was after the second accident that his opioid use ramped up and he got hooked.
During the discussion, Sherer spoke of how he bought opioids on the street to handle withdrawal symptoms when his doctor finally tried to get him off the prescriptions. [17:38] Over the next 9 to 10 years, Sherer was using a variety of prescription medications and street drugs. In 2016 he decided he'd had enough. He also concluded that self-medicating with cannabis would be his ticket out of opioids.
Shearer explained how using cannabis helped him overcome the physical symptoms of opioid withdrawal. He also believes cannabis saved his life. Had he continued using opioid pills and heroin, he believes he would have died from an overdose.
Today, he tells his story to anyone who wants to hear it. Tim and Chris are on board, being strong believers in Medical Cannabis as an exit drug. As a side note, the guys devoted part of the discussion to talking about prices and some of the other hiccups Utah's program is currently experiencing. [28:43] It was a great discussion all the way around.
Chris Holifield: So, this is going to be Episode 51, Tim.
Tim Pickett: I can't get over every time you say-
Chris Holifield: Every time you get on here, you get so excited. And you know what? I'm like a kid on Christmas to watch your face just smile, because I'm like, "Okay, this podcast is actually working." It's actually doing what it should be doing.
Tim Pickett: It's all because we have, really, it's all because we have you. You stick it out, you do it, you're good at this.
Chris Holifield: It's our community. Without our listeners though, we wouldn't have a podcast. So, really, you can say all that you want, but I'm going to thank our listeners for listening to the podcast every week, and downloading the show, leaving reviews, sending messages, all of that. So, who's on the show this week, Tim?
Tim Pickett: Derek Sherer, who is an exciting guest, but we've finally hooked up with him. And he has a fascinating story about addiction and cannabis. And I love stories like this, Chris, because they focus on cannabis being an exit drug, instead of a gateway drug. And that is the science is bearing that out. We have patients that are bearing that out. This is a good episode to listen to, for people who are seeking knowledge about the legitimacy of cannabis as something that can help people.
Chris Holifield: Absolutely, no, I was really excited to talk to Derek. And then, when I listen back to this episode, before publishing in here, I'm just like, "Wow, everybody's got to listen to this." This is a powerful episode.
Tim Pickett: Yeah.
Chris Holifield: So, hopefully, listen to the entire thing. Listen to it again. Share it with a friend. Share it with somebody who you might know is struggling with the same thing.
Tim Pickett: Absolutely. And we'll publish this on utahmarijuana.org/podcast, where we'll have a transcript and a summary, Episode 51. If you look there, all of our episodes there, remember if you want an update on the legislative session, and what's happening in the cannabis industry, Episode 50 with Rich Oborn was last week, which was a great episode.
Chris Holifield: So, good. Yeah.
Tim Pickett: Yeah. I'm excited to get into this with Derek. This is one that I think people should listen to, especially in Utah. This is a culture. It's a culture breakdown.
Chris Holifield: Very cool. Yeah. Let's get into this episode with Derek. Remember to subscribe to the podcast in whatever app you listen to this in. We have a brand-new episode, comes out every Friday, 4:20 AM. Let's get into that conversation with Derek. Thanks so much for listening. Here we go.
----
Derek Sherer: Congrats to you guys on the one-year anniversary. That's awesome.
Chris Holifield: Yeah, man.
Tim Pickett: Thank you, thank you, thank you. It's been-
Derek Sherer: Yeah, that's huge.
Tim Pickett: It's been an interesting year.
Derek Sherer: Yeah, it really truly has. Yeah. It's been nice to listen to, especially through 2020. You know what I mean? I fell back on your guys' podcast a lot just to escape and hear other people's stories. So, I'm loving it.
Tim Pickett: That's cool.
Derek Sherer: I'm honored to be here.
Tim Pickett: Thank you. Thank you. Well, I'm hoping to find out your cannabis story, and how you got... you're currently a patient, a medical cannabis patient. But how did you get introduced to cannabis? Let's go back to your beginning story, if you don't mind sharing that. I'm always curious the first time.
Derek Sherer: Yeah, yeah, of course. Yeah. Mine came a little bit later than most people. I did. smoke a joint with a couple friends when I was 15 years old. Didn't really spark any interest, no pun intended, but didn't really spark any interest to me. And passed it along. 17 years old, revisited it and really, really fell in love. Just with everything that it was, it was just, I don't know, love at first puff.
Derek Sherer: I guess you could say it, just I knew it was just something for me. I've never really been a big drinker. I have a family that's got a lot of alcoholism in it. Like to have a beer here and there and everything. But it's not something I see I could do every day, like a lot of other people do. So, yeah, this was just something that was for me. And yeah, 17, I know it's a lot older than a lot of other people you hear, all the 13-year-old, the 14-year-old stories and stuff. But quite a late bloomer.
Derek Sherer: And yeah, just really, really liked it from the beginning. I knew it was something that was for me. And then, I really wanted to educate myself on it more. I knew a lot of other people were just treating it like a have fun party type vibe. I really wanted to know more about it, and this is back in 2002, 2003. And it's just evolved so much, and I love learning more each and every day.
Tim Pickett: Yeah, you grew up in Utah too, right?
Derek Sherer: Yeah, yeah, born and raised here in Utah.
Tim Pickett: So, you said 17 is a late bloomer. Gosh, I was like 20 for the first time I-
Derek Sherer: Oh, really?
Tim Pickett: ... I smoked weed. Is 17 late? Is that considered late for people to consume-
Derek Sherer: For the stories that I have, yeah. A lot of people that I talk to, they are really super young. I hear some people talking 10 years old, 11 years old. I'm just like, "Wow." I'm thinking what I was doing around those ages. And it wasn't even a thought. You know what I mean? It wasn't a thought to me. But yeah, I get a lot of people saying that I was that late bloomer, and they're like, "Wow, 17, it's pretty old."
Tim Pickett: It's interesting that people have different... really, is it the world we live in now? Right, Chris? You, and I, and Derek, we live in this world where everybody around us uses cannabis. And it's just part of our life. And so, for you, Derek, to say, "Well, 17 is late." Well, in your world, I guess so. Right?
Derek Sherer: Right. Yeah.
Tim Pickett: But what's "normal?"
Derek Sherer: That is a great question. It really truly is. I got kids myself, so I would look at like, what is a good age for anybody to partake in any kind of thing like this? And what is normal? You're right. Because some other people see a younger version as normal, where others see, once your brain develops, obviously.
Tim Pickett: Right, right.
Derek Sherer: But yeah, what is normal I think changes day to day.
Tim Pickett: I'm going to be in that crowd, Derek.
Derek Sherer: Yeah, true, true.
Tim Pickett: When they’re 25, if my kids ever listen to this episode.
Derek Sherer: Yeah, mine too.
Tim Pickett: You can try cannabis when you're 25 children.
Derek Sherer: Exactly. Exactly.
Tim Pickett: Okay, not before.
Derek Sherer: Yeah.
Tim Pickett: We let that frontal lobe develop.
Derek Sherer: My kids too, yeah, they'll hear it.
Tim Pickett: But there are plenty of people who need an endocannabinoid stimulant-
Derek Sherer: Oh, 100%
Tim Pickett: ... before that. So, there are places for it before you're a fully functional adult.
Derek Sherer: Yeah. It does offer a lot. It offers so much. Like I mentioned, I educate myself so much, and dive so deep into stories. Obviously, like I said, I have kids. I've been an advocate for cannabis for so long. And then, I became a dad, and now I see myself as a dadvocate. I educate my kids.
Tim Pickett: That's a cool word.
Derek Sherer: Yeah, yeah. I like to educate my kids too. I have a 10-year-old and a five-year-old. They both, they know what daddy, what he does, they know what my passion is. They've sat down and watched stories, Charlotte's Web. The little girl Charlotte, this new one that we just seen that was called Waldo on Weed, really touching little story also. Six-month-old child that had a rare cancer in his eye. And parents picked up cannabis, CBD oil, and completely changed everything for this little boy.
Tim Pickett: Where's that video at?
Derek Sherer: You're right. It's called Waldo on Weed. I've seen it on Amazon Prime. The name itself just kind of pulls you, you see roots curling across, you see Waldo On Weed. It's like, "Oh, I got to check this out." It's a great story. I highly recommend it.
Tim Pickett: Yeah, I'm going to watch that after we're done here.
Derek Sherer: Yeah, It's amazing.
Tim Pickett: Yeah. I think you've got, when we talk about kids and stuff, I don't know if I can make a universal statement about this. But I'm trying to organize my thoughts here around it. Because you have cannabis, medical marijuana, you have alcohol, you have guns, you have sex, all of these four things that we talk about with kids. And it does seem like in every case, more education and more openness leads to better choices in general, right?
Derek Sherer: Absolutely.
Tim Pickett: You hide the booze from your kids, what do they do? They go try to find it. They drink. Hide the guns from your kids, you don't educate them about them. They go use them in bad ways. Same thing with medical cannabis, sex. Right?
Derek Sherer: Yes.
Tim Pickett: You taught classic for that discussion. We can't teach kids about sex education in school. We have to teach them about abstinence and what do we get? We get high pregnancy rates in teenage girls. Because we don't know how to use protection. So, cannabis is the same discussion. Be open with your kids about cannabis in a good way. Give me a good idea, Derek. Maybe we should write a book, a kid's book. What's in Grandma's Garden as a book?
Derek Sherer: Oh, man. I love it. Grandma's Garden. I love that.
Chris Holifield: Wait, is that a real book?
Tim Pickett: It really is. That's actually real book. You can go buy it on Amazon. What's Growing in Grandma's Garden?
Derek Sherer: You had me going there. I thought we had a deal working.
Tim Pickett: And it's a weed book, how to teach your kids about cannabis and-
Chris Holifield: It's awesome.
Tim Pickett: ... in a legitimate way.
Chris Holifield: That's awesome.
Derek Sherer: Yeah, I'm going to Amazon Prime that tonight, and maybe on the next book list.
Chris Holifield: When did cannabis come into your world, Derek? When did you realize you could use it on a medical level, more to help your body out instead of just recreationally?
Derek Sherer: This for me, I do fall victim to a lot of the... what a lot of people here in Utah fell victim to, a lot of the country in itself, the opioid epidemic. While back, a few years after high school, I'd say about 2006, 2007 was running with some wrong crowds, fighting, doing some damage to my hand, broke my hand three times, shattered it, required surgery on it.
Derek Sherer: They say it was too late, I'd done too much damage to it. Typical story, doctor was just pumping me full and full of so much medication that I didn't need. I was going and filling my prescriptions at pharmacies and the pharmacist was asking me, if you don't mind me asking what this is for, I'm telling this from my hand, and the pharmacist themselves are telling me this is way too much for you.
Derek Sherer: And younger kid right out of high school, I'm just like, I'm just taking what the doctor is prescribing me. Little did I know, it was creating massive damage to my body, to everything. I became so dependent on it, that's when the doctor was just like, "Okay, this is the amount of time, we're just going to take you off." There was no weaning off process.
Derek Sherer: My body became, obviously, I went through withdrawals, and had no idea. I never really been addicted to pills. I'd never known what that feeling was. Used cannabis recreational before that, I was really never too familiar with any other drugs besides alcohol. And didn't really know what that was doing at a young age. I was scared. So, I started looking for my medication elsewhere on the streets.
Derek Sherer: And at that point, I wasn't even helping the pain. I was just helping the pain from the withdrawals by seeking medication through the streets and everything. So, that had turned into a quite lengthy addiction.
Chris Holifield: How long ago was this for you?
Derek Sherer: So, this was 2007 when I got on the pills, for the second time, I'd seen two different doctors from two different breaks and shatters on my hand. The second one is one it just cranked up. The first one, I was on like some Percocet, some low-end stuff. Second one, it was oxycodone 80s, and it just got out of hand. And from about 2007 until about four years ago, I've been off everything opiates, clean for four years, all thanks to cannabis.
Derek Sherer: It just went downhill. And I've seen things in that time, and went through things. It was just no person should go through. It was losing at least two to three friends every six to seven months, it felt like, all the overdoses, all overdoses. I became numb to it. I had not lost a family member until I was like 26. But in that 26 years, I had lost at least 15 friends during that time, in just a short period of time, all to overdoses.
Derek Sherer: My parents, my dad still talks about it to this day that my friends have set a record for just bodies is going down on all to opiates. And yeah, cannabis was something that I had obviously used before. It's something that I use, obviously, just recreationally. Like I mentioned, I tried to educate myself on the benefits of it before, but never really knew the medical standpoint until I gave myself an option to look for other ways to get off this medication.
Derek Sherer: I did do the typical rehab. I went to rehab. That didn't work. I was doing Suboxone, methadone, terrified of that. I know they have the programs and it works for some people. But that stuff is just as hard to come off of as opiates are. And I think any person that's on that right now can tell me that's the truth too. So, cannabis was something that I really took a shot at.
Derek Sherer: I had tried so many different things. The Suboxone, rehabs, and just told myself, I'm going to have this pain, like the doctor said, I'll have this pain in my hand the rest of my life. That's just plain and simple. And in the wintertime, it gets even worse. Utah can be winter in March or winter in April. So, it's really hit and miss. But yeah, cannabis really stepped up for me, saved my life.
Derek Sherer: I truly believe it, and I owe it all to it. I educate a lot of other people that there's other options out there. And this is just, I feel like the best alternative for anybody that's looking to get off opiates.
Tim Pickett: How did you switch from opioids to cannabis? It sounds like you've been a cannabis user for a while, right?
Derek Sherer: Right.
Tim Pickett: And that's always been part of the equation. But at some point, there was this idea that look, I've got to get serious about getting off the opioids. I've got to get serious about using something else, or what does that look like?
Derek Sherer: Glad you asked, and by all means, I'm not ashamed of anything. I'm not here to glorify anything. The glory from my story comes from me getting out of it. Plain and simple. I tell this story to a lot of people because they ask, just like you did, how did you do it? I was so deep. I've tried so many different things. And what was the wake-up call?
Derek Sherer: I had switched from oxycodone just like a lot of other people to opiates to heroin was using intravenously, IVs, shooting up everything. And just this one day, it was just the weirdest thing. I still don't know what it was. I tell a lot of people this, they have their own thoughts on what it was. As I was ready to use again, I was just sitting there, and do you guys know the feeling like if you stand up too fast, you get tingling in your body?
Tim Pickett: Yeah.
Derek Sherer: Okay. So, I was sitting down, was completely fine, everything, not withdrawing or anything. And I could just feel that feeling going from my forehead all the way down my body just this tingle feeling. And it was like a snap of reality. And I just remember asking myself, is this it? Is this what you want to do the rest of your life? Is this for you? And I said, "Absolutely not."
Derek Sherer: I broke my needle off, threw it in the garbage, picked up some cannabis, and told myself I am going to beat this. I'm going to get through this. I told my mental state that it needs to take a backseat because I know a lot of it is mental when you're trying to get off opiates. A lot of it is obviously physical as well. But I truly believe if you can overcome the mental state, you can fight the hell out of it.
Derek Sherer: And I chose to, and through the withdrawals, through the pain that I was suffering, cannabis was the thing. I had my humor back. I was eating. I was sleeping. All of the things that a lot of these doctors can prescribe you. But there was no side effects from it. You know what I mean? There was really the side effects were hungry, happy, sleepy, all things that I could deal with.
Derek Sherer: All things that were just perfectly right up my alley. So, yeah, that was four years ago. 2016, November of 2016, November 27, and haven't looked back since. And cannabis has been not only the thing for me, I've helped a lot of other friends that have been in need. I know a lot of people see me, and they're like, "Wow, he did it." And they have questions. And that's the only answer I can give them. I don't know what else it was. I don't know if I would have made it without it. I truly, truly don't.
Tim Pickett: Tell me why do people go to heroin from the pills? How does that happen?
Derek Sherer: That transition came honestly, I can almost remember the day, oxycodone really took off. I can't remember around what year it was. But it really took off and was just creating damage everywhere. All over from every corner of the country. And I remember when they took it off the shelves, and the company just said we're done with this. It was like Willy Wonka's golden ticket.
Derek Sherer: Nobody could find them and everything. So, that was a huge transition for everybody is that that became unavailable. So, somebody else just said, "Hey, I have this other thing. Cheaper, and just as strong." And so, once that settles in, it's just off to the races with that.
Tim Pickett: I've heard the same thing. It's actually just cheaper.
Derek Sherer: Yeah. Oh, yeah. Completely, completely.
Tim Pickett: It's like, it's easier to get in some ways, and it's just plain cheaper. You can't afford the pills, so you got to switch to heroin.
Derek Sherer: Yeah, yeah. And it's dangerous. But even more now, though, with the fentanyl that's came in. I'm just so glad I got out when I did. It's a blessing.
Tim Pickett: It's interesting too, how people can label marijuana as a gateway drug when you're using it to get off of drugs. It's like how does-
Derek Sherer: It's an exit, yeah, it truly is.
Tim Pickett: Why can't we get people thinking that way, I guess?
Derek Sherer: I've thought that for the longest time, and you know when you have one of those ideas, and then you're just like, this is such a great idea, and then you go to look it up, or you don't even go to look it up, and then you just see your idea. They have a facility. I've always thought that for these drug and rehab facilities that they're giving people, they give people methadone, Suboxone to help them detox.
Derek Sherer: I've always thought: why has no one ever tried cannabis to give these patients? There's a place in, I believe it's California called THC, The Heavenly Center. A music producer, Scott Storch helped fund it, and everything, and they use specific cannabis to get people off. Matter of fact, I've just seen today, there's a center here in Utah that I believe is doing that now.
Derek Sherer: That is introducing medical cannabis to people who are trying to get off opiates. So, it's amazing to see that people are taking a shot at it because I truly haven't seen it fail. I'm a person that's speaking the truth from it, and anybody else who has taken my advice, they're right here with me. And it's a blessing to see. Every time that I can see how it can heal anybody, it warms my heart. It truly, truly does.
Tim Pickett: What's the difference between the high associated with the opioids or heroin, and the feeling of cannabis? Because I've talked to some people who've come off of alcohol, and they'll say, "Well, I still get that craving and it's different." It's not the same relief as the alcohol is. How does that work with cannabis and opioids, or cannabis and heroin?
Derek Sherer: Yeah, it's a good question. Honestly, for the longest time, and this is probably true for a lot of users, I was never really getting high in the end. I was just getting by, and I was just getting better. A lot of addicts would chase that high. I never wanted to chase it too much, because that's how you overdose. You can overdose off of a small amount, but a lot of people would chase it so much, and push the limit.
Derek Sherer: It was just to get by for me. It was really not necessarily taking away any pain. It wasn't giving too much euphoria. But I do remember smoking cannabis while I was in the midst of an addiction, while I was in the middle of it. And just to quote Bob Marley on it, when he says the cannabis helps reveal you to yourself. I remember smoking while I was just got done getting high off opiates, smoking some cannabis and thinking to myself, why am I doing this?
Derek Sherer: Why am I using these opiates? I would literally have conversations with myself. And think this is so stupid. And I was so close to like, those were the close times that I had to full on stopping and quitting. So, I knew that when I had that rollover and just said, "Hey, is this it for you?" I knew that hey, every single time before you smoked, you would always ask yourself, you really got back to you. And it was the truth.
Derek Sherer: So, there was really not much more of a difference. I would say credit definitely would go to cannabis. It would obviously get you high, but it wouldn't... to me, it was just more of a spiritual type thing. It was more of this is real, this is safe. There's more of that hug high, more than that, like you're just out of that kind of high. I felt the embrace every single time. But sometimes the opioids were really too strong in the moment. But since then, yeah, like I said, it's a blessing. It truly is.
Tim Pickett: Now that you know what this process looked like for you, think about all of the knowledge of cannabis. You started when you're 17. You're in your mid-30s now. You've come a long ways. You've learned so much about cannabis. Could you design a program better now to get somebody like you, could you go back to you and be like, "Hey, four years ago, you'd be like, hey, man, Derek, you know what? You're using this strain. No, no, no, you need to be using this in the morning. You need to be using this at night. You need to be using this tincture here." What's that look like now that you know?
Derek Sherer: Now that I know, I just want to know more. I truly, truly do. I believe I've become such an advocate, and such a promoter for this that a lot of people around me to talk about different things, whether it'd be neuropathy, whether it'd be diabetes, whether it'd be pain, whether it'd be anxiety. I feel like I am starting to educate other people on what, hey, this is what you need. Hey, maybe you need CBD. You don't need THC. Maybe you need some CBG. You know what I mean?
Derek Sherer: For inflammation. There's a lot of different things. So, I'm more trying to create this program for myself to help others to really pass the message of cannabis on, not only just for myself, for the loved ones around me, but for my kids. I truly, like what we were talking about in the beginning, what is normal for a child to start taking something like this? I can see my kids taking CBD at a very young age, given if they need it.
Derek Sherer: There's just a lot of options outside of Big Pharma that people need to take a look at, and they don't need to see this as a last resort. It's very tough for me to hear when people are suffering through certain things that they say we don't have any other choice. So, we're going to try this. This is our last resort. So, we're going to try cannabis. It's tough to hear. It's also good that they're giving it a shot, but this needs to be the frontline. It really needs to be the frontline.
Tim Pickett: Top three, instead of the bottom.
Derek Sherer: Hands down.
Tim Pickett: Right.
Chris Holifield: What's your favorite way to consume cannabis? What's your favorite way there?
Derek Sherer: I've always been into the art form of a lot of different things. I used to roll sushi and everything like that. Rolling joints was a thing of mine. That's for me, and my friends in the past, we tried to roll the best, and everything. I really do enjoy the vaping now. To me, back then, it was when somebody had a vape it's like no, what are you talking about? But there's so many benefits from it, from the vaping. Edibles, I've really trained my body on them, more or less.
Derek Sherer: I'm understanding a lot about how they work with metabolism, with lots of different things that you eat. So, that's interesting to start working on the doses on that. But just really all things. There're so many different things that work on so many different levels. But yeah, for me, I love the taste of the flower. I'm a flower child at heart, really. I love where cannabis is going, extracts, tinctures, I love where it's going, but more kind of the old school flower child.
Tim Pickett: Yeah, there's something about it, Chris. There's something about the flower.
Chris Holifield: Just that right stickiness and just that-
Derek Sherer: It is. It's the beauty. The beauty of it. There's so much.
Chris Holifield: Right. There's that experience of grinding it, of rolling it, or of putting it in the vape if that's the way you consume it. Certainly, there's a lot of people who still smoke it in Utah, even though it's really outlawed. But yeah, that's the thing, would you want to grow it or no?
Derek Sherer: Yeah. It's always been a dream of mine, it really has, and especially with what I've been talking about is offering this as another alternative. I would love to figure out the perfect, I know there's great strains out there for people that are coming off of opiates, but just one that's just going to be the end-all be-all that a lot of other people can say this is going to be the one. You're coming off of opiates, not Suboxone, not methadone. It's this particular strain.
Chris Holifield: Yeah, that is a high goal.
Derek Sherer: It really is.
Chris Holifield: That's a really cool project, though.
Derek Sherer: Yeah, it really is.
Chris Holifield: The right ratio of cannabinoids, even down to that where you're going, "Okay, maybe we don't need a 30% THC strain, we need 12%, we need high CBD."
Derek Sherer: High CBD. Yeah.
Chris Holifield: We need that anti-anxiety.
Derek Sherer: Somewhere around the lines of the ACDC strain. I know that that's a one-to-one strain that's rare out there with higher CBD.
Chris Holifield: I've never seen it.
Derek Sherer: Right. Yeah. And you don't, and you don't. A lot of people are just-
Chris Holifield: You don't see it.
Derek Sherer: ... high THC. They just want them 30 percenters, and there's more benefits in CBD, CBG, CBN, so many different things that people need to take a look at.
Chris Holifield: I know, it's always interesting in a lot of the online forums, people get so bent out of shape about the whole of low THC, the flower in Utah is just too low. And I'm just like, "I don't know, it's not all that bad."
Tim Pickett: We had some we had some discussions today with Justice Grown and they're talking about this program as a real medical... this is a really medical program and medical programs, they're not the same as adult use programs. We are not going to have the same products that they have in Colorado. We're just not.
Chris Holifield: They just need to bring that price down, though. That's hard to keep it as a medical thing, because it's like people can't even afford it.
Derek Sherer: Yeah, I feel real bad for a lot of the indigent patients out there that some of these prices, man, I work and I have kids, and everything like that. My dispensary buys just are just enough. But yeah, it is high. I'm just thankful It's here. I truly am. I remember watching when Prop 2 was getting passed, I literally was up refreshing my phone all through the night, all through the night. Like come on, come on, come on, come on. And bless that it's here.
Derek Sherer: There's a lot of kinks in the system and in the program right now, but I'm very hopeful that they're going to get it worked out. I think it's just going to get better. But yeah, prices, it would be great. IAND I was really looking forward to, if patients were able to grow because that is just a huge thing. I heard you guys' Bob Waters episode. Shout out to Bob Waters, that thing, that was amazing. I would love to get in touch with him. So, if we can link that up like that was-
Tim Pickett: But he brings up a good point, right? It's $24,000 for his medicine per year. And it's not covered by insurance. And it's like 20 bucks to grow his medicine.
Derek Sherer: Yeah. And I thought about that, that 24,000 and it just made me think like, "Wow, how much is mine?" That number just put out there like his is a lot, but some are probably a lot more. But still just a lot of money in itself.
Tim Pickett: And people are going to look at that, and they're going to say, well, it's like a bad habit. They're going to compare it to smoking cigarettes. If you quit smoking cigarettes, you'll save all this money. That's different. It's a medicine. It's not the same thing, right?
Derek Sherer: It is, right.
Tim Pickett: We have people with chronic pain that require this substance. And we subsidize that with insurance for all other medications, but we have no way of subsidizing it for cannabis, right?
Derek Sherer: Yeah. It's just amazing. If people were able to grow it, I think it would just... it's so much more of a benefit. Just being around the plant, I'm sure you guys have felt that change, and just being around the plant, you just feel a difference and everything. But yeah, it's medicine. And if a person can grow their own medicine, why not? You know what I mean? I wish diabetics could make their own insulin. That would be amazing. There're just certain things, it's like, why restrict those things? But again, I don't know. It's new.
Tim Pickett: Yeah. We're not the people who make the rules. We've got to live by those rules.
Chris Holifield: Hopefully. Hopefully, one day here in Utah, they'll at least allow the people that are way out in the boonies, allow them to at least grow.
Tim Pickett: Yeah. And I think it's my understanding, there's going to be another retail license that gets out there. And that's supposed to be designed for the rural market, so that there's more access in those parts of the state that really have had a hard time with access so far. Because if you look at where you've got to travel to, anywhere south of Provo, you got to go to Provo, you got to go to Deseret Wellness. There isn't anybody south of there. There will be, but still, man, it's a long time coming to get these guys open.
Chris Holifield: Yeah. The program has been up for a little over a year now. And so, it's yeah, all those patients down there. You're pretty much forcing them to cross state lines. And it's a terrible thing. It's a terrible thing. You think of all these people that have never broken a law in their lives, willing to risk their lives to go get their medicine across state lines, because they have no other way. That's a terrifying thing to think of.
Tim Pickett: Sure. And this is legitimate. You talk about coming off of opioids. And I can talk about 70% of my patients are reducing their other medications, by using cannabis as an adjunct, as an addition to their medications. It's a big deal. We want more of that data. We want to drill down on that, but that's a huge number.
Derek Sherer: Completely.
Tim Pickett: Seven out of 10 people using less other medications, whether that's alcohol, opioids, sleep Ambien, with less long term side effects, in most cases than the other harsh, harsh medication. But then again, the issue is price. You got to go buy it on your own. You can't even use tax deductible funds, like your health savings account to go buy it.
Derek Sherer: Yeah. Little things like that that would really step up and make a big difference. Yeah, and people are going to have to start looking at this. I know probably, medications are a little bit cheaper. Yes, you can use your insurance, but 2020 itself, I can see a lot of mental illness coming out from a year alone, and people requiring cannabis. That was a tough year for everybody. Everybody should have got a qualifying condition card just that year alone, just to help us through it.
Tim Pickett: Right. Like if you survived 2020, you qualify.
Derek Sherer: Yes, yes.
Tim Pickett: That should have been in the legislature.
Derek Sherer: Completely, completely.
Tim Pickett: I love it. The 2020 qualifier.
Derek Sherer: Yeah, it should be, it should be a qualifier for everybody. Because yeah, it's something that people really need to open their eyes on. It's not the taboo dope that it used to be before, and I know that people used to throw that word around, and call cannabis dope. And that's probably one of the biggest pet peeves of mine. It's not. It's so much more. And it's on its way. I'm happy to see it, always happy to share my story with anybody.
Derek Sherer: And anybody who's suffering, who hears this or anything like that, they can feel free to reach out to me because I'm always there to talk. But just like I tell everybody, I'm in it as much as you are. I'll help you as much as you want to help yourself. Because it has to come from within. A lot of people are scared. But there's better options for everybody. And this was the one for me that completely saved my life.
Tim Pickett: What about your family and friends? Are they pretty supportive of you using cannabis or do you keep it hush hush?
Derek Sherer: You know a great question. My mom and dad, bless their hearts for going through what I went through and everything. It's something no parent should have to go through having a child as an addict. It's terrible, but we made it through it. And they're huge, huge supporters. My mom was really the... it's drugs, she's never taken drugs in her life, never smoked a cigarette, she has wine from time to time and everything, real, strait-laced upbringing, and everything.
Derek Sherer: So, something like what I was going through and cannabis, it was just all wrong and all bad. So, she got to see what I went through. And she got to see what cannabis did, and she complete, I can't even say the word 180, it's an understatement. She's so supportive of it. It warms my heart just to hear how onboard she is with it. She tells people how much it saved my life.
Derek Sherer: She's fully supportive. She doesn't look at it differently now. Years ago, if she would have found out how I educate my kids on it, she would like, wow, they're absolutely not so wrong. But yeah, my mom, she was the biggest change. My dad has always been supportive. He uses it himself, also for his depression, and everything. But for her, she didn't understand it.
Derek Sherer: She never understood the benefits of it. My friends, yeah, they see what it did for me. So, they have no choice, but to see that it helped. They always have questions about it. Tim was talking about what strain did you use and everything. And at that time, I was getting it from friends. But that's the great thing now is I know exactly what to use.
Derek Sherer: So, it can help a lot of other people by educating them. But I do have a couple family members that are, how do I really put it, not necessarily judgmental towards the fact, but they don't understand it. They're not educated themselves yet. And that's all I can say about it is that they just don't know enough to fully understand what it's doing. They've always seen other things as other options.
Derek Sherer: So, they still don't believe that this is the end-all be-all for me or anybody else. But yeah, for the most part, everybody is super, super supportive. They know how passionate I am about it. My kids constantly asking me different things. We watch shows, like I was mentioning before. So, yeah, full-on support from those around me.
Chris Holifield: I love it.
Tim Pickett: Yeah, that's pretty cool. And I think that the family members, you talk about who aren't supportive, you're right. It's this really, a lack of education, but it's got to be a lack of willingness to admit, or to maybe not admit is the right word. But it's this understanding that you don't know. This this acknowledgement of something you don't know about. And so, I'm going to go out and find out about this, right?
Derek Sherer: Yeah, yeah.
Tim Pickett: It's thinking, and I guess that's judgmental to say, yeah, if you don't think cannabis can be medicine, then you think you know, but kind of you really don't. You got to be willing to learn.
Derek Sherer: Yeah. These are the same people that are the wine versus weed kind of things. They partake quite a bit in the alcohol, and see that as, "Hey, it's right, what I'm doing, it's legal what I'm doing. Well, it's also legal what I'm doing also." But this is something that's new that you guys have seen taboo for so long. I don't like to get in debates too much.
Derek Sherer: But it's something that I will always debate people on, I feel. I feel like I'll always stick up for cannabis. And I can argue with everybody, but what good does it really do for somebody who doesn't really want to learn themselves? Alcohol, you look up top 10 dangerous drugs in the world. Alcohol will be top three in every single list that you find. You will never see cannabis close to-
Chris Holifield: Yet alcohol is legal.
Derek Sherer: But it's legal.
Tim Pickett: Yeah, but alcohol is legal. To turn this a little bit, do you feel like there's some danger to excessive cannabis use? Do you feel like people can get into using too much, and really not be good for their health? Do you feel like you ever got into that spot?
Derek Sherer: Great question. I don't feel that I've ever really got into it myself. I'm a firm believer and that it's really not for everybody. But at the same time, I fight that it's not for everybody, because I think for the person that tries something that experiences something bad, whether it's high anxiety, paranoia, you just hear all these stories where it's just a terrible experience, or they use in an excess, and something changes.
Derek Sherer: I think those people need to be educated on what they're using, and maybe find out what we're talking about, what works best for them. Maybe you're taking a 30% when you don't need a 30%. You need something lower. Maybe you don't even need THC. Maybe you just need CBD. I understand people play with cannabis as it's like alcohol, so people will partake in it just for fun. But at that point, also, it's still good to educate yourself on what you're using.
Tim Pickett: Yeah. You don't — you don't go to the bar and just say, "Hey, just light me up."
Derek Sherer: Yeah, you don't, you don't.
Tim Pickett: "Give me three hits of that."
Derek Sherer: Exactly. Great. Yeah, great.
Tim Pickett: You're right. You order a drink because you know what's in it, you know the taste.
Derek Sherer: You know, exactly.
Tim Pickett: Right. It's the same. It's got to be the same a cannabis from a recreational standpoint, right?
Derek Sherer: Absolutely, absolutely.
Tim Pickett: You got know what you're doing. And I bring that question up, because I do think in my opinion, there is an access to cannabis use. I think people can use too much. I've definitely met some patients who, in my opinion, they use too much. If you're using a gram a day, and you don't have serious cancer pain, or something, man, lowering your tolerance could be beneficial to your health.
Tim Pickett: So, this balance, cannabis is a substance, the endocannabinoid system is a system that tries to find that balance. That's really what we're trying to do with medical cannabis is we're trying to bring the body back to homeostasis, that evenness. And so, I think that in any case, and the Mormon Church is really into this with the word of wisdom, and that is finding this balance, no excess.
Tim Pickett: So, I don't know, I'm getting a little on my soapbox here. But I think you can use too much. But on the other hand, educating yourself about what to use and how to use it. That's okay. That's a good thing for people.
Derek Sherer: Absolutely. Anything can be used in excessive points. It comes down to personal control at that point. But yeah, I 100% agree that people need to know exactly what they're using, because that's when I think it can get out of control and out of hand. It doesn't even become medicine at that point. You're just rolling the dice, and just figuring out, "Hey, let's see where this goes, and let's see where it takes you." Just like you said, here, bartender, fill me up. Nobody does that.
Tim Pickett: Right. You don't know what-
Chris Holifield: Surprise me. Surprise me.
Derek Sherer: Yeah, nobody does that.
Tim Pickett: That's a bad idea. Yeah. That's a bad idea for no matter what you do. So, now, you've come all this way, what's next for Derek? because I know you're really now working in the industry.
Derek Sherer: Yeah, I am.
Tim Pickett: Is that what's next?
Derek Sherer: Yeah. It's a blessing. I don't even feel that I go to work every day now. I truly don't, and I know that it's a blessing all around. My kids see this excitement, my fiancé sees this new side. It's just what's next for me is just to keep on going, keep educating myself, and I would love to continue to help educate other people as to, like we talked about, cannabis is not the entrance drug.
Derek Sherer: It is the exit from a lot of things. And people need to look at it different. So, what's next for me? The sky is the limit with this. I truly feel more at home being in this industry than I've ever felt in anything in my life. You can ask my dad. It's been a struggle for him, I've had every job underneath the sun trying to find my way, trying to find my home, and this is it. So, I'm just going to continue to grow, no pun intended, or pun intended, because I may be growing one day.
Derek Sherer: But yeah, I know that this is something that is it's beneficial for me in so many ways other than just being a medicine. I love being around it. I love educating people. I love what you guys do. This type of podcast is so needed to educate people from all stories that you guys have, business people to patients to whoever. Everybody needs to tell their story about how this has helped change, shifted, done anything in their lives because this is a life-changing situation.
Derek Sherer: And being in the industry itself is life changing for me. This is a career. This is not a job to brag about. I'm not just a pothead trying to make a point. I'm here to help heal, and educate, and show people that it works because I wouldn't be here having this conversation with you great fellows if it wasn't for cannabis. It's a fact.
Chris Holifield: I'm grateful for cannabis. I'm glad to be sitting here with you chatting and finding your story, man.
Derek Sherer: Appreciate it.
Chris Holifield: Are you on Instagram? Can any of our listeners connect with you through Instagram, or anything, or do you have a website, or let's share some of that information?
Derek Sherer: Yeah, I am on Instagram. It's DJ_Deuce, D-E-U-C-E, 801 (@dj_deuce801). One of my other passions, DJ and stuff. So, yeah, I'm on Instagram. And like I mentioned, anybody who's going through the struggles can definitely reach out. I'm always happy to lend an ear, to help out.
Chris Holifield: Yeah. I'm going to get you on our Facebook patients' group if that's okay.
Derek Sherer: Absolutely.
Chris Holifield: And then, utahmarijuana.org, we've got a Facebook group, a patients' group that people can reach out to others, and in just get a sense of what this is like for somebody else, get a little bit of back and forth. I think a lot of people, they need that here. There's a little bit of isolation here, especially. You don't want to go talking to your neighbors in some cases.
Derek Sherer: Yeah. It's hard. It's hard to reach out. It was hard for me. I had to reach out to my inner self and have that conversation with me. But yeah, I'm always here for anybody who needs the help.
Chris Holifield: Yeah. Cool. So glad I brought you on the podcast or that we brought you on the podcast.
Derek Sherer: Yeah. The take two. The take two.
Chris Holifield: Yeah. I know it's been a couple of times. Last week, we tried, but my internet was out. I apologize about that.
Derek Sherer: Yeah, it's all good, it's all good. I like the take twos. The number two is very synonymous in my life. So, it fits now. So, I'm happy.
Chris Holifield: Perfect. Very cool. Well, anything else you want to ask him, Tim, or anything else you want to bring up, Derek, before we wrap this episode up, or anything?
Derek Sherer: No, I think I'm good. Again, congrats to the one year. You guys are doing an amazing thing. I literally can't get enough of this podcast, and listening, and shout out to everybody who's been on here. I enjoyed all the stories all across and always looking forward for more.
Chris Holifield: Maybe eventually, one day, we can get everybody together, and we can all just have a big day and vape together, right?
Derek Sherer: Hey, that'd be awesome. Looking forward for that.
Chris Holifield: [crosstalk 00:47:09] but we can't do that here in Utah.
Tim Pickett: Yeah, I'm thinking 4/20/2022.
Derek Sherer: Oh, I like it. I like it.
Chris Holifield: Oh, man, we better have a 420-party when-
Derek Sherer: Yes, we should.
Tim Pickett: Just a little while longer.
Chris Holifield: Very cool. And everybody can go listen to all the other episodes of the podcast at utahmarijuana.org/podcast. You can listen to them right on the website, or you can subscribe to the podcast in whatever podcast app you listen to all your other podcasts in, and leave a review if you haven't left a review in Apple Podcast, or wherever you listen to podcasts. Anything else you guys want to say, or let's wrap this episode up, and go on with our lives, I guess?
Tim Pickett: Yeah, I guess so. Well, thanks everybody for listening.
Derek Sherer: Of course, shout out to everybody in the industry, everybody in my work, you know you who are. You guys have a great night. Keep on doing what you're doing.
Tim Pickett: Stay safe out there, guys.
We are always on the lookout for news about the Medical Cannabis space in Utah. Back in mid-December, we learned of new legislation being proposed for the 2021 session that would, among other things, make it possible for pharmacies to store large quantities of product in warehouses so that they could deliver directly to patients. Home delivery would be a big step forward for Utah patients.
With that said, imagine our delight upon stumbling across a Salt Lake Tribune article published January 21. The article details the efforts of a Utah dispensary that has begun home delivery to patients in fifteen counties, including Wasatch and Salt Lake. The company has hired ten couriers already.
That's fantastic! Home delivery is just what Utah patients need until there are enough brick-and-mortar dispensaries to serve everyone with a reasonable level of convenience. Moreover, it is critical to patients who are too ill or fragile to make the trip to a dispensary.
Home delivery does a lot of good things, including:
It is not clear to us how this new home delivery service squares with the previously mentioned legislation. At this point it doesn't matter a whole lot. The fact is that patients in fifteen counties can now have their Medical Cannabis delivered to them.
We hope that this is just the start of home delivery. Utah is a mostly rural state. As you know, driving into Salt Lake City or Provo can be quite an undertaking for some residents. Others cannot do it at all. They either have to send a qualified caregiver to go in their place or do without. That's not good.
We need more access in rural areas, that's for sure. We need ways to reach those patients who have no other option for getting Medical Cannabis. Here's hoping the proposed legislation makes the complete rounds and eventually lands on the governor's desk.
In the meantime, the doctors here at utahmarijuana.org are ready to help you obtain a Medical Cannabis card. We invite you to make an appointment to visit any of our clinics at your earliest convenience. You can schedule an appointment online or call 801-851-5554.
Obtaining a Medical Cannabis Card is not as hard as you might think. You visit with a qualified medical provider (QMP) to talk about your medical condition. Hopefully, that means coming in and speaking to one of our providers. But either way, the QMP can determine if your condition qualifies for Medical Cannabis under Utah law.
Assuming that is the case, the QMP will fill out the necessary paperwork. You submit that paperwork along with your application and the associated fee. It is then up to the state to review the paperwork and approve you for a card. That's really all there is to it.
Just remember that Medical Cannabis Cards are not permanent. They do have to be renewed from time to time. Often, this does mean a return visit to the QMP. But that is nothing to worry about either; the process is as simple and straightforward as can be.
Utah has taken a huge step forward with the introduction of home delivery. Here's hoping that legislators will approve the warehousing plan so that dispensaries can get Medical Cannabis products to patients all over the state. The move would be a life-changing one for countless numbers of patients.
The Department of Health's Rich Oborn joins Tim and Chris for episode 50 of Utah in the Weeds. This might be the most important episode thus far for those keenly interested in legal aspects of Utah's Medical Cannabis program. Suffice it to say that the latest legislative session has brought significant changes that all Medical Cannabis patients should be aware of.
The two most significant changes involve the expansion of access to medical providers and the implementation of the controlled substance database. In terms of the former, new rules will allow any medical provider with a controlled substance license to recommend Medical Cannabis to up to fifteen patients without having to get directly involved with the state. [42:14] Pharmacies will handle EVS reporting in such cases.
In terms of the controlled substance database, it is a done deal. [5150] Information on patient use of Medical Cannabis will be entered into the database along with all other controlled substances. Medical providers and clinics will have access to the data at any time.
Other legislative changes include:
Episode 50 is longer than most Utah in the Weeds episodes. It is packed with valuable information you don't want to miss. Listen closely to the details and be aware that many of the changes being brought to bear will not be implemented immediately. Some will, but others will not be implemented for weeks or months.
Chris Holifield: All right, well, this is Episode 50 of Utah in the Weeds. My name is Chris Holifield.
Tim Pickett: And I'm Tim Pickett. Congratulations, Chris, on making it to Episode 50.
Chris Holifield: Episode 50.
Tim Pickett: Yeah, I mean every time we record lately — we've had the year anniversary. And now we're having Episode 50. And we've had and today's guest is Rich Oborn, the head of the Department of Health, the Utah Medical Cannabis Program for the Department of Health. And here we are talking to him for the second time, which is perfect for Episode 50. Right?
Chris Holifield: Yeah.
Tim Pickett: And we've been in this program for a whole year. There's just so many things that seem like they're getting better.
Chris Holifield: When we talk about that in this episode, some of the changes with the laws… a lot of good information. Listen to the whole thing, it gets a little long.
Tim Pickett: It does. This is a long episode. But I think it's worth it. This is the legislative update basically for what's going to change in the Utah cannabis program for patients, for providers, for pharmacies. And there's a lot of little tweaks that were made over the session.
Chris Holifield: And what I enjoyed talking with Rich here, Tim, is there was a lot of things that I was kind of first like, "I don't like that." But then with some clarification, I was like, "Well, that's not really that bad of a law really."
Tim Pickett: Right. He does bring it. He brings some context to some of these changes.
Chris Holifield: Yeah, I'm like, "Okay, that makes sense."
Tim Pickett: Which I think is good. I mean he runs a reasonable department, and the Department of Health has been extremely helpful for patients. And anyway, this is a good episode. I encourage people to listen all the way to the end, because there's good things all the way right up until the end.
Chris Holifield: Listen to the end, make sure you're subscribed to the podcast in whatever podcast player and utahmarijuana.org/podcast is where you can get all the other podcasts.
Tim Pickett: That's right. And we're going to put a summary of this podcast on utahmarijuana.org/podcast. If you look for this episode, Episode 50, you'll have a link to a blog post. We'll put it up. And we'll run through those legislative changes if you want to find out more.
Chris Holifield: Or follow along while we're talking.
Tim Pickett: Yep, exactly.
Chris Holifield: There, go to the website, boom, follow along. And that way you guys can be up to date and find out what's going on, because it's important as medical cannabis users to stay up to date on all the laws.
Tim Pickett: I think especially because this is still federally illegal, you really want to be, you want to pay attention. There's information about the controlled substance database. We talk about that towards the end. And I think that's one of the big things that patients need to pay attention to. Let's get into this conversation with Rich Oborn.
Chris Holifield: All right guys, here we go.
-----
Chris Holifield: So there's 24,000 patients in Utah, cannabis patients?
Rich Oborn: Active registered patients in the state of Utah.
Chris Holifield: 24,000.
Rich Oborn: Over 24,000. So we're working on 25,000. It increases every day, the number of active patients in the program.
Chris Holifield: And did you expect what? 6,000?
Rich Oborn: No, I think it's important to focus on the fact that when we projected things, there are certain timeframes in which we thought we would have, and 6,000 was the amount of patients that we thought we'd have by July 2020, because March 2020 is when the program rolled out. And 6,000 sounds like that number is-
Tim Pickett: I remember somebody was saying that, yeah.
Chris Holifield: And I had read 16,000 the first 12 months based on some Arizona numbers, something like that.
Rich Oborn: Right, right, and that was high. And it was all based upon what other states had experienced, because that's the best data we had. But what we've experienced is a growth rate that has been higher than has been seen in other states, which is great for the program, for patients. We didn't expect that our growth rate would be bigger than what other states had at the very beginning. And it took time to get there. But once we adjusted and moved forward, we really saw those numbers increase, especially at the beginning of the year, or actually at the end of 2020, when everybody started to hear that recommendation letters were going to expire and they had to be a registered patient with the Department of Health in order to purchase product. So yeah, there's so many factors that impact but here we are, over 24,000 patients.
Tim Pickett: Yeah, I mean it's really, it's a good system in the making. There's still some kinks to work out, and we're going to talk to you about that and go through some of these legislative changes and not only what's happened over the course of the year, but what we think will make the program better for patients over the course of 2021. Of course, having access to more pharmacies was a huge deal in 2020, and product. And maybe we should just go down kind of this list just to kind of keep it organized.
Tim Pickett: But really, we have this, the legislature passed a 15th —or they're going to allow a 15th retail location. Is that just going to be another pharmacy? Is it going to be something different, some type of hybrid?
Rich Oborn: It will be a brick and mortar 15th pharmacy, and we're excited that it will be dedicated to a rural area. It has to be in Daggett, Duschene. You went to Sevier, Grand, San Juan, Emery or Carbon County, central Utah. San Juan, I suppose, is also southern Utah. It's a giant county. But I would say there's some cities within those counties that are more frequented than other cities, higher population like Vernal or Price or Moab or Richfield, the applicants for those, for that 15th license, they'll propose a specific address that will be in one of those cities. And we'll take a look at the strength of those applications and we'll compare them with a point system that's fair and balanced.
Rich Oborn: And so just because one pharmacy may stick out from another in one category, it doesn't mean they're going to win at all. We got to be balanced in how we review, and I think we expect to get some really strong applicants that we're looking forward to reviewing. It's a request for proposal, an RFP that has to be submitted. So it has to go through what's called the Division of Purchasing with the state of Utah. And that ensures one reason why it's going through that process is that just ensures that the process will be fair and balanced, and that there's a fair and balanced award system for points as they go through that process.
Tim Pickett: Because I'd imagine this is going to be pretty competitive. I mean, you're only issuing one more license. There isn't really anything on the horizon that says Utah needs another four or five licenses for a little while. I mean, do you see that there's, does Utah project the need for more than 15 for a while or is that even not on the radar?
Rich Oborn: I think what we've focused on is we need to see what happens with all the 15.
Tim Pickett: Once 15 go in?
Rich Oborn: Right, because we've got eight open right now. The next one to open will likely be Beehive Farmacy in Brigham City. And we have pharmacies open up in places like Springville and-
Tim Pickett: Columbia, Springville.
Rich Oborn: The city of St. George and South Jordan, and those haven't opened yet. And so I think that those are critical factors that haven't fallen yet that will help us learn more about the market and the need for potential additional locations. The law already provides the Department of Health the ability to consult with the Department of Agriculture to determine if additional pharmacy locations are warranted. We don't have to go to the legislature for that.
Tim Pickett: So anytime you could just be like, "Hey, we need a 16th pharmacy, boom."
Rich Oborn: Yes, but we need to establish criteria. And we'll be working with the industry to establish that. That hasn't been established yet, just because we know that all the pharmacies haven't opened up yet. And the past year, there's been-
Tim Pickett: They're not near to capacity, right? I mean, some of these places can do 600 or 700 transactions a day. And there's nobody doing that many transactions a day yet.
Rich Oborn: Right. And something also that's critical that has rolled out not to the extent we need it to in order to understand the market better is home delivery. Yes, there are some pharmacies that are much further along than others. Two are approved to do it, two of the 14.
Tim Pickett: So you've got a Wholesome who's been doing home delivery up from Bountiful, and I think Dragonfly, they've opened it up too, but that's not to say there isn't, certainly Deseret has talked about doing home delivery, and that's going to be a big deal. And that could expand the reach of these pharmacies into other areas and decrease the need. What you're alluding to is that could decrease the need for additional licenses.
Rich Oborn: Potentially, but something else we want to be having a pulse on is the need for an individual to meet in person with a medical provider. And we want to, if they want that, if that's just their preference, then we want to consider that in deciding whether or not we approve an additional brick and mortar to be in some of these rural areas where they simply just don't have that option under even 15. They have to drive over 100 miles in order to get that option to meet in person. There's always this offer for counseling with a pharmacist that could happen over the phone, and that's being taken advantage of already. And that could just expand even more. But for some people, they just prefer to meet in person. They want to be able to see that person, different approaches to getting cares to patient. And it's important to respond to some of those demands.
Tim Pickett: Well, we see it in medicine, too. I mean, telemedicine really took off during the pandemic. But the truth is, there are patients who just want to come see you face to face. And there are times when you really just need to see the person face to face and look them in the eyes and see how they're walking and how they're doing. And so yeah, I mean I can appreciate the idea of needing, potentially needing more spots.
Tim Pickett: When you talk about the pharmacies that are going to open now, the legislature adjusted the timeframe, the time to open. Did they give them a little leeway there?
Rich Oborn: More specific about what that timeframe is. There was a little gap in the law previously and what the SB 192 did is it set that deadline at June 1, 2021. And the prior law just had a little gap. So that was addressed by this absolute deadline of June 1, 2021. And all the pharmacies have confirmed that it's definitely a deadline they can meet, those that haven't opened yet. So we'll see St. George, Cedar City, Springville. And there's one im-
Tim Pickett: Well, Cedar City's Bloom. So you've had yeah, I mean, I've personally talked to Bloom. They want to open. Of course, they want to open by end of April. Justice in St. George, I was actually down there. And they also want to open by April, they got a lot of work to do in those places.
Rich Oborn: Columbia Care in South Jordan.
Tim Pickett: Oh, yes in South Jordan. That's Justice off of 106 or so, where their location will be, and that will be really good to have more locations. I can't imagine being in southern Utah, and not having access to a location now. I think that's tough. But also, the legislature adjusted the rules for possessing cannabis. Was that to kind of cover? Talk to us a little bit about that. Was that to kind of cover that extension to June 1.
Rich Oborn: Yeah, that was the logic behind it is just to give patients I think, especially in those areas where they don't have as much access, the ability to continue to possess out of state product legally. In some cases, it's really important. Also, I think it's important to keep in mind that the supply and the variety of products, I think has improved. We expect more improvement, as any new program would with medical cannabis. And I expected during the summer, it would have improved to a point where it's just not nearly as much of a problem as it has been in the past for supply and variety. Naturally, one of the frustrations from patients has been that there hasn't been the supply and variety, and from the companies, that's been one of their frustrations as well. But everybody who knows cannabis knows that every program has started this way, especially in a program that has started as regulated as ours in the type of atmosphere that it's just had to grow in. So that additional time was given I believe for those reasons.
Tim Pickett: Yeah, I mean, it looks here like you can, so patients can possess out of state product within Utah as long as they're a medical patient and they have a card until June 30 of this year.
Chris Holifield: That's if the products comply though with Utah. You can't bring in like THC drinks and stuff like that.
Rich Oborn: You've never been able to do that.
Chris Holifield: Well that's what I'm saying, so people listening-
Tim Pickett: Okay, guys. you can't go get edibles.
Chris Holifield: And I don't think a lot of people know that, Rich because I see a lot of, Facebook groups online. I'm like, "Man, these people must not know the laws.", because I'm just like, "Man."
Rich Oborn: Yeah, it's important that people educate themselves and if they have questions to talk to people they trust that know the law like an attorney or just someone that works in the industry, so they are aware of those limitations of the type of products that they can possess. Even when you do purchase out of state, you need to make sure you're in compliance.
Tim Pickett: We even have a kind of a rule change within the system now, right? There's been gelatinous cubes with sugar coating. And evidently like the Department of Health, with the industry is kind of adjusting things as they go. That specifically comes up on the Facebook groups and things like this, the sugar coated gelatinous cubes.
Rich Oborn: Right. That was something that was tracked by the Utah Department of Agriculture and Food because they deal with the processors and cultivators. As a Department of Health representative, I deal with specifically the pharmacies and what ends up at the pharmacy. But I do know that the Department of Agriculture and Food did see that happening. And they I think gave a deadline by which the pharmacy would have to stop selling those type of products. They didn't say you have to stop this immediately. They gave them a time.
Tim Pickett: They just said, "Hey, this doesn't really meet what the rules say as far as gelatinous cube." And so I think that some of the products, I know I talked to Zion, the thing about individually wrapping every cube, and there'll be things like that. I think that's kind of me personally, I think that's kind of silly, but I don't know.
Rich Oborn: It's nice to have it individually wrapped like a Starburst or something.
Tim Pickett: Right, and they wrap those. And the other thing about those gelatinous cubes is if they're all together, they tend to melt. So you got, I mean, one way or the other, you got to keep them separated.
Rich Oborn: Yeah.
Chris Holifield: What else have we got on this list here? I mean, I got a bunch of stuff here.
Tim Pickett: Man, we got a lot. The collection of QMP medical clinic fee data, oh yeah, and this involves me. So this healthcare transparency idea that we need to be as transparent as possible, and we're going to supply, we're going to supply the government, the state government with fee data. What's the reasoning behind this?
Rich Oborn: It's something similar to what happens with the payers claims database. And if you know something about Medicare, you might know that there's certain types of facilities that have to report what their fees are to the Department of Health already in the all payer claims database. Those fees are collected. And it's a complex, it's a complex system. It's not as simple as just collecting a fee. There's different things that impact what that looks like. But the State Auditor's Office today, if you go there, you'll find that there's this healthcare transparency tool that exists already for Medicare purposes, for medical providers where they have to report this different types of facilities already do this for those other purposes. And it's already a tool that's used by patients, if they know about it, to help them decide where to go get service. Now, it is, I think-
Tim Pickett: Is this something like okay, look, I'm going to go get a hip replaced. And so at this hospital, I can look up on the database, and I can kind of figure out that it's going to cost about $25,000. But if I go to this other hospital, then the fees end up being $42,000, and that's kind of the idea?
Rich Oborn: Right, so Senator Escamilla, what she wanted to do is to reflect that type of a transparency tool for medical cannabis patients specifically. And I think one of the issues that we found early in the program is naturally there's a limited supply, or limited number of qualified medical providers. Many of those choose to not have their information posted publicly. They would rather just continue to meet with their current patients, and that's their choice. So their name doesn't appear on our website. You wouldn't really know that they provide medical cannabis recommendations as a service, unless you're one of their current patients. Maybe they're an oncologist or a neurologist and they have that specialty.
Tim Pickett: Yeah, not especially new patients, but they'll do medical cannabis recommendations in the course of their own practice.
Rich Oborn: Right. So those type of providers aren't required to post what their prices are, for purposes of medical cannabis evaluations. The type of providers that are required and the type of medical clinics that would need to make sure that their providers report would be those that advertise publicly like your medical clinic, that they do provide medical cannabis evaluations. And there has been some concern of some of the prices that are charged because the number of those type of medical clinics is limited at the beginning of the program. There's a wide variety of prices that are charged, and in some cases, the legislature believed that they were charging too much. Rather than saying you cannot charge over a certain price, the legislature says, "Okay, free market, you do this. But we will require that if you advertise that you provide medical cannabis evaluations, that you communicate those to the Department of Health, who will ensure that those prices that you report are posted on a health transparency tool online the cannabis patient can use as a resource to confirm the price that they would be charged." Now, there's a lot of different factors that impact price.
Tim Pickett: There is a lot of different factors.
Rich Oborn: That's the biggest picture, just that one little slice of the price, right?
Tim Pickett: Yeah, that's right.
Rich Oborn: So I know you'd probably want to talk about that a little bit?
Tim Pickett: Well, yeah, I think that there is there is a lot and there are going to be, of course, there will be clinics that will lower their initial price and lower their initial, the care they give the patient. And unfortunately, fortunately, unfortunately, that's part of the marketplace in all businesses. And I think that hopefully, patients, the bottom line is hopefully, patients will do their research on who they're going to see and they can look at this tool and they can say, "Okay, you know what? I'm going to look at these places, and I know what the prices are going to be. But then I'm going to dig in a little bit more. And I'm going to find out a little bit more about the reviews and who's gone to see them. Are these people giving me the service that I am really paying for."
Tim Pickett: That's really all my concern is when it comes down to putting these prices online, because they're certainly going to be and there are plenty of places out there that are just like, they're the card mills that everybody doesn't like. You're really paying for a recommendation at something like that. And with me, you're paying for an evaluation, a lot of education, a lot of follow up. Maybe you get what you pay for in a lot of places. So do I agree with the legislation in the way it is? No, but will we do it and will we go out of our way to make sure the patients know what they're getting? Absolutely. And in that case, it is what it is.
Rich Oborn: One thing I think is important for cardholders, patients out there to understand is that this isn't something that we are immediately requiring. We need time to set up the software in what we call an API integration, to set up our software so it can connect with the state auditor software. So I would expect that this will be rolled out in the fall. It's not something to expect immediately. But it's something that will change in the future that I think will empower patients, but they need to just be aware that price shouldn't be the only factor and that they need to keep those other factors in mind that you mentioned.
Tim Pickett: Yeah, absolutely. When we talk about the, oh yes, it's the 90 day renewal in the conditional card. This is like a huge thing.
Rich Oborn: But these are good things.
Tim Pickett: Yeah, I think they're really good things. So talk about the legislation surrounding this conditional card, this provisional, they're calling it a provisional card. So are we going back to the letter system?
Rich Oborn: No, we are not going back to the recommendation letter system. So there continues to be a requirement that to legally possess and to purchase product, you must be a registered medical cannabis card, active card holding individual so you cannot possess or purchase product without a medical cannabis card that's been issued by the Department of Health. But one of the things we learned as we move forward in the program is that we believed we could trust the relationship between a provider and their patient. And as long as a provider made the clinical decision to certify the recommendation of someone to give them a medical cannabis card, as long as that was in place, that we could allow for a conditional card to be issued. And that card, the purpose of it would be to give, it's conditional because the final decision about the card hasn't been made. But it just gives the state time to ensure that an appropriate review has occurred on the state's end to ensure that everything is accurate, and there's no fraud taking place that would be evident in the online application.
Tim Pickett: This is a really good-
Rich Oborn: So allowing the patient to go and purchase, but we always have the right within that timeframe to take the card back to revoke it if we notice that there's something funny going on.
Tim Pickett: Right, some box wasn't checked. The clinical documentation wasn't there, something was missing. But this, in my opinion, is just smart legislating of actually, and I think I mean as rare as that sounds, that you get a government that is, is doing something that is really smart. This is one of those things where you've seen 18,000 in 2020, 18,000 applications come across the Department of Health, the EVS system. And you can tell of those 18,000, or however many you did, how many were revoked or how many needed more information. And then you can make a good determination, plus you had the letter, recommendation letter system that already we had gone through. And we had kind of proven as a early system, that we could evaluate patients and give them access to the product. They could go purchase it. And that turned out to be a pretty good, safe system.
Tim Pickett: There was problems with that. But it was, let's say safe. And now you've made a change that continues that process in a really good way. I think it's great for patients, because it was one of the big things in January and February that we were asked, "Don't you do the recommendation, Tim?" And we're like, "Well, yes. But then you got to wait.", and recently, the Department of Health has been a little bit behind. You're caught up now. But it's great to have people be able to leave the office with that recommendation and go down to the pharmacy. How long will that take to implement? There's the question.
Rich Oborn: I think we're looking at fall 2021 for that type of the lift. That will be to our software vendor that we're working with. So we're really excited about it. I think one thing that's great about an online system is that it can be smart, and it knows when a patient, by the information that's being provided by the provider and the patient, it can make those automated decisions about who should get a card and who shouldn't. We're not pushing paper. We're able to prepare the system so it can automate some of that process like an e-script would.
Tim Pickett: Right, you're sending across the recommendation, just like an e-prescribed medication. And that's being verified by however many factors it is. You verify me, I verify the patient, they're already registered. Yeah, it seems like this is a good, this is going to be good for patients, right? Chris, I mean when you think, now will this happen do you think with renewals? If somebody expires, will they be able to renew their card and immediately be active? That may be a detail you don't know yet, but is it the same type of thing?
Rich Oborn: Right, right. Same process for renewal. It will be an automatic issuance of a conditional upon renewal. And then that individual, as soon as the providers, as you do that certification, the system will read that and then issue a conditional card. And then we'll make sure that everything is on the back end like it should be. And then we'll then issue the second email with the card because all these cards are sent via email. We don't send one in the mail, except for when people request it if they don't have a printer or whatever, we help them out.
Tim Pickett: But that's not really part of the program. How often does that happen where people really need a physical card?
Rich Oborn: Oh, I'd say people, we have probably every two weeks, maybe three, where people just request that, and that's fine.
Tim Pickett: Yeah, we probably have three a month that come into clinic and want us to print it. So it happens. Yeah, we'll print the card.
Chris Holifield: And laminate it too?
Tim Pickett: We need a laminator. No, we will laminate it for them.
Rich Oborn: I think one thing to focus on as we think about how this will benefit patients a little bit is that the 90 day period of the initial issuance and renewal cycle is gone in the new law. It will take time for us to implement the software changes.
Tim Pickett: Right. Because right now, the software automatically creates a 90 day-
Rich Oborn: It's a 90 day. That will continue until the fall, because we need time for our software to make those changes and several other changes, including this one, but it will benefit patients and providers, because I think it will honor the relationship that they have that's critical, that there continue to be a provider involved in the treatment. But rather than 90 days, it will be six months for that initial issuance. There's the conditional card that is for 60 days. But then, as long as the department does our part to ensure that everything's in there, then it will be for six months. So there won't be the need for the user provider to meet with a patient after those initial 90 days again. It will be a six month period.
Tim Pickett: I'm torn about this one, Rich. I'm torn about the 90 day going away. I know it will save us a lot of work. And I know that it will save the patients a lot of headache. A lot of patients, it will save a lot of headache. But there has been a very good relationship built, I think on that. This is why I'm torn. And there's been an opportunity for us to follow up with the patients at 90 days. And when you do a cash pay clinic, or you do a clinic where patients are having to pay out of pocket, and then you don't charge for that 90 day renewal like we don't, it allowed us an opportunity to research how the patients are doing and things like that. And so, like I say, I like the idea of not having that. We're actually going to see the patient sooner than we would have before because right now, we're seeing them in about eight months. And we will be seeing them in about six, about five or six. So we'll still be able to see them. It will change that a little bit.
Tim Pickett: So I think overall good. But yeah, I'm a little torn, because I like getting that feedback from the patient sooner.
Chris Holifield: Or you can keep doing it.
Tim Pickett: And I still, yeah we still-
Rich Oborn: As a medical clinic, you can shorten that time period.
Chris Holifield: You can still do it if you want.
Tim Pickett: Yeah, and we have and I think we'll find ways to follow up with patients and do that. But I think overall, it's going to be nice for the patients to have a little more clear, you get your card, your card is good for six months, your card is good for another six months. And then we can start to work on this, whether or not a year is good for the patient. And that's kind of the idea behind this change, is that right?
Rich Oborn: Yes. Another change that's coming up is there's a prohibition against alteration or removal of a medical cannabis product label that came from the processor.
Chris Holifield: I thought that was already.
Rich Oborn: Right. So this was just clarifying that I think we wanted to make it really clear that-
Chris Holifield: You're talking about the labels you get when you go to the pharmacy with that-
Rich Oborn: It's on the actual product you purchase.
Tim Pickett: Yeah, okay so it's actually the label on the jar, now there's a going to be a rule that says you can't remove that.
Rich Oborn: Right.
Tim Pickett: Why is that important?
Chris Holifield: It's like a mattress label, right?
Rich Oborn: That helps protect the patient, if by chance they're pulled over by law enforcement, law enforcement can track down that product to make sure that it was a legally purchased product. Also, for recall, if there's a problem with the actual product and the patient experiences and adverse reaction. If you keep the label, it allows us to research how many other patients might have been impacted by that same product that had an issue.
Chris Holifield: My question though is sometimes you might buy a few small ones and put in a big one, put it into a big jar at the store. And then if you don't have-
Tim Pickett: Yeah, I mean if you bought a couple of eights, and you had a little bit of a jar-
Chris Holifield: Yeah, you might throw them all together.
Tim Pickett: So now you got to be careful.
Chris Holifield: Maybe save all your empty containers, I guess.
Rich Oborn: This law, what it does is it focuses on the alteration or removal of the actual label. And part of it has to do, I think it's applicable more to cases where you're transporting product if you're going back and forth to work with it.
Chris Holifield: I got you, I got you.
Rich Oborn: Right? Because those are cases where you would actually potentially be pulled over, and if that becomes an issue, cardholders need to know.
Chris Holifield: They need to be able to identify themselves, show what they have.
Rich Oborn: Right, if that becomes an issue. It may not, but part of it is just to prepare a patient and a law enforcement representative to be able to, as a patient, protect themselves and as a law enforcement representative, to investigate. It makes that process quicker.
Chris Holifield: See, that's why I like you on the podcast here because you can kind of clarify things.
Tim Pickett: That's right. I mean it's because I think a lot of people are just going to look at that and be like, "Yeah, that's silly." There's no reason behind that, but yeah, I mean it makes okay, yeah, these guys are thinking this through before they just willy-nilly change the rules.
Chris Holifield: I want to talk about this one on here, though. It's the one that says a pharmacy medical provider must review each medical cannabis transaction. So each time you purchase something at a pharmacy, you're going to have to have a pharmacist there to review it?
Rich Oborn: Right, so already, a medical cannabis pharmacy during all business hours has to have a pharmacist, or they call it a pharmacy medical provider physically present during all business hours. That's already a requirement in Utah, and it's in other states like Minnesota and Connecticut as well. So that's already been a requirement. But one thing, one critical role that a pharmacist in a retail pharmacy like a Walgreens plays is they are responsible for any differences between a prescription and what the patient actually leaves the pharmacy with. A critical role that pharmacist plays is just being responsible for what's dispensed. That's the verb that's used to describe that responsibility in a regular retail pharmacy.
Tim Pickett: You're talking about at the end of the transaction, when I buy my amoxicillin, the pharmacist, there's the pharmacy tech that does the whole thing. But then at the end, the pharmacist comes up and grabs the medication and says, "Hey, I'm going to double check that. Do you have any questions for me?"
Rich Oborn: And a lot of time, you don't see how that happens right there exactly. But especially with controlled substances, you'd see how important that is with opiates and narcotics before it's dispensed, to ensure that the patient is actually getting something that is consistent with the prescription. So that's what happens in a regular retail pharmacy. Now, we're going into a medical cannabis pharmacy that naturally has some differences in how things happen. But there are some things that the policymakers felt very strongly about. And one of those things is if there is a recommendation from the qualified medical provider like Tim, and when they purchase a product with that recommendation, is that recommendation being followed? Are the dosing guidelines or directions of use that have been communicated by Tim in our software being followed?
Tim Pickett: No.
Rich Oborn: And the legislature wanted to emphasize the need to ensure that a pharmacist is involved in making sure that actually happens in a medical cannabis pharmacy like it does in a retail pharmacy. The pharmacist is responsible to ensure that whatever is recommended as a dosing guideline is actually followed. And also keep in mind that a qualified medical provider can choose to leave those dosing guidelines and directions of use up to the pharmacist at the medical cannabis pharmacy, which is good.
Tim Pickett: And even more so now, yeah, it is good. And maybe even more so now with some of the modifications that we can talk about next. And I guess it will take a little time for the pharmacists and the pharmacies to get this in place to where this is a little bit, this is smooth for the patients, right?
Rich Oborn: Right.
Tim Pickett: I kind of look at this particular rule as a doubling down. The legislature is kind of doubling down on the medical aspect of this program.
Rich Oborn: Yeah. And in their words, I think they are just emphasizing their original intent. They intend for a pharmacist to operate in a medical cannabis pharmacy, just as they do in a regular Walgreens retail pharmacy, just like they do in Connecticut and Minnesota. And they wanted to clarify that that is their intent in the law. So now it's very clear what their intent is. And now as the Department of Health, we are working with, I was just speaking with one of the medical cannabis pharmacies today about how to implement this. And so I think we'll work out those plans in the best way. There's in the short term, how it will be implemented. And in the long term, the long term will have the software revised so it will be able to make it really seamless and easy. The short term, that will be a little bit more of a challenge, but in a retail pharmacy, it happens. So let's take that model and mirror it in a regular medical cannabis pharmacy setting.
Tim Pickett: When does that take effect? Is that taking effect more immediate? That's something that they'll have to, these pharmacies are going to have to abide by pretty soon, right?
Rich Oborn: Yeah. So the governor actually still hasn't signed the bill, either HB 170 or SB, it's SB 170 and SB 192. That will happen later this week. There's no reason why I believe he wouldn't sign these bills. So they become effective upon the governor's signature. But as a regulatory agency, we're reasonable. We don't expect, like a light switch for pharmacies to be able to implement things upon the switch. So actually, we're having conversations with pharmacies, even today about how to implement things in the short term. And we don't have a specific date yet. But it's something that patients I think should be aware of, because what may begin to happen is that they may go in and experience where they want a certain product. But if the pharmacy medical provider, the pharmacist that's physically present there, has a recommendation that doesn't quite match up with what the patient wants, then the pharmacy is obligated to limit their purchase to what has been recommended by either the qualified medical provider, or if there weren't any recommendations of dosing guidelines or directions of use, the recommendation of that pharmacist at that facility.
Rich Oborn: So that is something that they need to keep in mind, because they'll experience that it will be happening more often, that there could be that difference. In most cases, I don't think it will be an issue, because I believe the pharmacies right now are ensuring that that happens. This just makes it more clear. It gave us some teeth in the law to educate the pharmacies about, and it gave us the ability to require something in the process, where a pharmacist would be required to show the Department of Health, "Here's evidence that I approved what that patient actually ended up with in the end.", that the pharmacy agent wasn't running the whole show until the end, that there was actually a pharmacist involved. Because after all, this is a medical only program. And I think that's reflected in this emphasizing of the need to dispense accurately, and not just to sell whatever the patient wants.
Tim Pickett: Right. So the law also changed, and is now going to allow every medical provider with a controlled substance license to write recommendations for up to 15 of their patients. Right?
Rich Oborn: Right.
Tim Pickett: And in this they had to change, it looks like they had to change the way that was done because those providers aren't going to be required to input the information into EVS. The pharmacy looks like they'll be the ones entering those patients. Am I right about this?
Rich Oborn: Yes.
Tim Pickett: So with this rule, is this rule designed to kind of expand maybe rural access or access? How did this come about?
Rich Oborn: I think there's a few reasons for this amendment to the Medical Cannabis Act. One is, is that if I've been someone that is a patient that is treated for chronic pain, and I really trust my provider, and man, chronic pain sure is messing up my life, why would I want to change my provider?
Tim Pickett: Why would I want to go somewhere else, pay money if I can stay right here?
Rich Oborn: Right, and I love the fee that they charge, they take my insurance and it's convenient. It's just down the road. Why would I want to drive 100 miles to somebody else?
Tim Pickett: And then if we role play this, I would say as the provider, really I'm not somebody who wants to get involved in cannabis in a big way. But I know you, you're a patient, it's probably reasonable you tried cannabis. I don't know a lot about it. Now, I'll write the recommendation.
Rich Oborn: Yeah. So this law, it gives the option to any physician, APRN, PA or podiatrist that was-
Tim Pickett: Oh yeah. And they're adding all podiatrists into the Medical Cannabis Act, which is a good idea. They went to medical school.
Rich Oborn: So as long as you are in one of those license groups, and as long as you have a controlled substance license, then you could participate in recommending, ordering the pharmacy to help your patient get a medical cannabis card.
Tim Pickett: You're essentially writing an order for the pharmacy. You clarified that in a good way. You're essentially writing an order that the pharmacy help this patient, get a card, get a recommendation and work through that process.
Rich Oborn: Yes. So what's critical is that the pharmacy be prepared to accept that order. Now, there's certain information that appears on a prescription for a controlled substance, the name of the doctor, their controlled substances license number, their professional license number. One thing in addition that these orders will need to include is the medical condition, because that will need to be entered into the electronic verification system that represents, the pharmacy kind of works as an agent of the physician. The physician really doesn't want to work with the electronic verification system so they just authorize the pharmacy agent or pharmacist at this particular pharmacy to act as their agent in entering this critical information into the software database that then triggers the issuance of a medical cannabis card to the patient. So it would make it so I could just stick with my provider, as long as that provider agrees to make that recommendation for me. The provider will have to do a little bit education on the pharmacies, and the pharmacies will be able to set up their own ways for that order to be communicated either electronically or on paper. If it's on paper, then there'll will need to be a verifying of that, actually, the legitimacy of that order directly with the medical clinic or provider that submitted the paper order. So that is how it will work.
Tim Pickett: This seems like it's going to be another one of those kind of upgrades and modifications in the EVS system to change to create a new role, so to speak as the provider, a tier two provider, let's say or something like that, somebody with only 15 of these, and you got to follow them a little more. Is it going to be more work for the Department of Health for these types of in this system with these types of patients? Do you foresee that this will be more work for the Department of Health?
Rich Oborn: Yes, not an enormous amount of work. But there's some additional oversight that we'll need to create. One thing that's critical is that we set up a software in a database that is able to do a lot of the work for us. If we can trust it to set certain rules and to allow us to go and audit the software, then great. Let's automate things to make things as easy as possible. So that's critical. And I want to emphasize this is a good example of something that will not be rolled out really soon, the limited medical provider role will be something that it will require until the fall at the least for us to roll out. So again, a lot of these changes we've been talking about, they're not able to be actually implemented until we have the software to support it. But once we get that software in place, it will I think provide some better options for patients, especially in this one case where they're able to just stay with their current provider, which I think is the best type of circumstance as long as the provider feels comfortable recommending and ordering a pharmacy.
Tim Pickett: Yeah, to do this with them. I mean, I think I'd give a little bit of my opinion here. And I hope people expect that a little bit from me at this point. The more research I do about cannabis, and the more I learn about cannabis medicine, the more I see that having a relationship, when it comes to true medical marijuana treatment, having a relationship with a medical provider, whether it be the pharmacy medical provider, or a QMP or somebody who you trust, helping with dosing and delivery discussions who knows the patient's condition well enough to know and cannabis well enough to know what to recommend, the outcomes seem to be better when you have that relationship.
Tim Pickett: So while I agree with increasing patient access with this modification of the bill, I hope that the providers who are going to do this are willing to learn enough about medical cannabis to move forward in their own education, because I think the patients get more benefit when somebody knows what they're talking about when they're doing the dosing.
Tim Pickett: And I think the pharmacists have a role to play there too. Of course, you know, I'm going to be biased and say, "Look, I like our process." But this is an interesting experiment, I think, and I've talked to Ray Ward about it too. And that idea of trying to bring these other providers into the fold of agreeing that this is medicine and it's okay, it's just another tool in the toolbox. It's a complicated tool. It takes a while to get good at using it. But I agree the more providers that we get involved and get more education, the more likely it is we're going to see cannabis used in the hospital. And that really is the end goal. So yeah, I like and dislike this one. And I think that it's going to be more work, obviously more work for the pharmacies, a little more work for the Department of Health. And we'll kind of see, we'll kind of have to see how this goes. Maybe we'll bring on a doc in a year, who decided, "Hey, I'm going to write one of these recommendations.", and then all of a sudden realized, "Oh my gosh, I prescribed less opioids. My patients are coming off their benzos. It's actually working."
Rich Oborn: And I think one thing a lot of us are looking forward to is when the federal government makes research more possible when we can get more FDA approved drugs that have gone through the traditional process and where a traditional doctor would obviously trust that it would be sold by a regular retail pharmacy. But of course, the law is still what it is. It's still federally illegal if it has 0.3% or more THC, then it's still federally illegal and you've got this patchwork of 35 states or so that Utah-
Tim Pickett: That have different programs. And they all have a little bit different programs all the way around, right?
Chris Holifield: What else have we got on this list?
Tim Pickett: So the controlled substance database, the privacy, so it ended up passing, right? Okay, well, the people won in a lot of ways, and maybe we lost in this one. So now, the controlled substance database, will it be patient's information is going to be going on to the controlled substance database. Will it be tied into the EVS system? Is that just how it's going to be built? How is this going to actually work?
Rich Oborn: Yeah, so there's a few different databases. There's what we call the EVS. That's the patient registration system. There's the ICS. That's the seed to sale software database.
Tim Pickett: That's MJ Freeway?
Rich Oborn: Yep, that's MJ Freeway. And then there's also in this, particular to this amendment to the law, the controlled substance database for Utah. Every state has a controlled substance database, or they call it a prescription monitoring program in other states, and in about 15 other states that have medical cannabis, they incorporate already medical cannabis product information. And legislators thought, "Hey, we want the providers that are participating in the program to be able to be aware of the medical cannabis products that are being purchased and whether or not their particular patient is a participant in the program."
Tim Pickett: Okay, so basically, somebody comes into the ER, when I'm working a shift. I drug test the patient for whatever. They have THC in the system. I look them up in the controlled substance database. They're not registered. Then I could essentially tell that patient's not a member of the program and they're using, well they're essentially using it illegally. Is that part of this?
Rich Oborn: That's one part of it. Yeah, that's part of it.
Tim Pickett: I mean it's kind of an example.
Rich Oborn: Through your lens.
Tim Pickett: Right through my lens, because I still work some in the ER, and I'm trying to imagine how we're going to use this, and I can see exactly how-
Chris Holifield: What good would it be? So what if they're using it illegally? I mean, what are you going to do? Throw them in jail in that case? Or what would that do?
Tim Pickett: No, because my experience is patients are discriminated against when they use marijuana products. And that's just, I mean, that's just my experience, I would have guessed that that would be borne out by some type of studies or research but when somebody comes in and a provider has a bias against marijuana, cannabis use in general, drug screening them is a way to discriminate essentially. And so I don't want that. It was one of the arguments against using the, putting this data into the controlled substance database. However, there are some, being able to see that a patient comes up THC positive and is in the controlled substance database, if I'm a provider that doesn't have a QMP license, now I've protected the patient from discrimination. So as much as I just made an argument against, I'm making an argument for the patient in this case, because now the patient is actually protected and they can say, "Well, I prove it. I'm in the CSD and I came up positive." Well, it's no wonder.
Rich Oborn: Right. So another I'd say advantage of this and one reason why I think legislators are so strongly supportive of it was because this will allow, let's say I go to my chronic pain physician isn't interested at all in recommending medical cannabis. So I go to a medical clinic that's separate, to get a recommendation for my medical cannabis. This initial provider that was treating me for my chronic pain, if I continue to go to that provider, that provider would be able to see that indeed, "Oh, okay, I see you're a legal patient in Utah's program. And I can see what products you're purchasing. Interesting, I can see your frequency as well of purchasing A, B and C products." And I think it will give that provider a complete picture of how that patient is treating their chronic pain, has chosen to treat their chronic pain that they may not otherwise have.
Tim Pickett: This is objective data that I'm interested in, because we have had a number of patients who, although most pain providers do urine test pretty frequently, we've had a number of patients that have come through to us where they'll get, they'll qualify certainly. And they want to reduce their opioid use. And they'll start using medical cannabis, but they are afraid of being cut off from their provider. So I can see this working a little bit of both ways. I think the important thing with this one is that if you are a medical cannabis patient and you're listening to this, and you have a pain contract with a pain provider, you need to be aware when this takes effect, that this is going to be the source of truth for the providers. And they will be able to see all of the controlled substances that you're using, which is we check the controlled substance database when patients come in for medical cannabis. That's requirement by the statute. So we get all the truth. But we also don't, we don't broadcast that back to whoever. If the patient requests that that information doesn't go back to their provider, then it doesn't go back there. But now that will be available.
Rich Oborn: Right. And so I think one factor is just thinking about the need for continuity of care. And if I were a physician, I'd be able to ensure that I'm aware of the all the controlled substances, including those that are federally illegal, like medical cannabis, that they're taking. Now, if they're buying off the black market, you wouldn't see that of course. You could be able to see that oh, this patient is a medical cannabis cardholder, their card is active, but nothing's showing up. And that may tell the story of if the patient's using, then they're probably buying off the black market, especially after July 2021 when it's illegal to possess product.
Tim Pickett: What do you think about all this, Chris? As somebody who's outside of this, what do you think? Do you think this is just flat out an invasion of privacy? Or you think-
Chris Holifield: This particular thing?
Tim Pickett: Yeah, this particular thing.
Chris Holifield: My first thought was invasion of privacy, but after discussing it and after hearing some of these other angles, I'm like, "Okay, that makes sense." I mean, especially if you kind of want to regulate a little bit and keep an eye on things. I think it could be a good thing, but it could also be, I don't know if I'd say a bad thing, but it could be, it could cause some-
Tim Pickett: This is going to cause some anxiety in certain people.
Chris Holifield: Yeah, yeah.
Tim Pickett: And it's going to be, I guess it just comes down to how it's used. It really depends on the provider, the type of relationship you have with the patient. It encourages certainly honesty. It definitely should encourage honesty between the provider and the patient and what is happening. And I think that as we move this movement of de-prescribing, I don't know if you've ever seen this hashtag around, but it is a growing movement that really, we've started to become a big part of this de-prescribing movement and using cannabis as a tool to de-prescribe-
Chris Holifield: Opiates-
Tim Pickett: Opioids and benzos, gabapentin, Ambien, these things that just treat symptoms. They don't treat disease. They just treat symptoms. And cannabis is similar but may have less long term negative side effects. And so this controlled substance database, in that sense could help.
Chris Holifield: I just don't like being on any databases. So the thought of putting people on that, you know what I mean? Like the less, but at the same time, it's kind of like, well it is what it is, the EVS system I mean already has I guess all the patient's information too. So I mean, the information's out there.
Rich Oborn: Right. Yeah, I'd say that just an additional advantage to think about is just the ability for the provider to do research. We've got one of the best world class medical institutions here in the state of Utah at the University of Utah, right? So they want to do research. And they want to know what's the impact on use of medical cannabis on opiate use. So we've got data that tracks both for specific people that can be protected and be kept confidential. But there's ways with this connection to protect that data, but at the same time, use it for research that's legitimate. And so that's one thing that I think excites some of the individuals that were behind this is that it just allows them to do that research with the approval of what's called an institutional review board to ensure that patient confidentiality is always protected and there aren't a bunch of files going around with patient names on it.
Tim Pickett: Right, because essentially, what you're saying is I could take, if I'm the University of Utah, and I get permission, I could take data based on 2020 opioid prescriptions in Utah. And then I could take, once I get access to this, I could compare that to opioid prescriptions in 2022 now that we have cannabis, and we're researching that.
Rich Oborn: Right, and even look at specific records of unique identifying individuals. And take a look at oh, we noticed that this individual, as they use medical cannabis, their prescriptions-
Tim Pickett: Of other controlled substances-
Rich Oborn: Other controlled substances decrease. Now, there's research out there already. Some of it suggests that they decrease. Some of it suggests that over time, it actually that is not the case. It depends on a lot of different factors. And we need to be careful with making conclusions on the current research about that. But this just strengthens the ability for researchers to be able to take a look at that over time, and then to publish studies in the future, that Utah could really be, I think a model for that, depending on how things move forward with the University of Utah in their interest in doing some of the research. The funding is tricky for that type of research. That's quality research, where they have to spend a lot of time crunching numbers and doing all that that I'm not the expert on. But it just requires funding. And it can't be federal funding because of the fact that-
Tim Pickett: Because you're studying federally illegal substance still, but you're studying a federally illegal substance in the best way you can, which is this.
Rich Oborn: Yes. So the controlled substance database and the inclusion of the medical cannabis product information, I think has that potential benefit.
Tim Pickett: So overall, do you feel like the legislative session was a success for patients, for providers, for pharmacies, for the program?
Rich Oborn: It definitely was. I think there are a few things where we have yet to see. And that's part of what the legislature's job is, is to say, "Okay, let's just see if this little tweak makes it a more pleasant experience for patients.
Tim Pickett: I like that.
Rich Oborn: Right?
Tim Pickett: Right.
Rich Oborn: Or makes it just a little easier for provider to be involved in the continuity of care of their current patient. What tools can we create? So policymakers approach it like that. I think it was, that's something that Senator Escamilla and Senator Vickers were looking at and Representative Ward and Representative Gibson is a sponsor of these two bills. Now, there's some other bills that impact the agriculture side of things, a little bit more with hemp, and I know that that's something that some people listening may have interest in as well. But I'm not an expert on those issues. But as far as the medical cannabis patients go, I think it was definitely progress. And as we learn more about the program, I think we'll be able to even make further tweaks. We are excited to continue to launch the program. Full launch hasn't happened yet. We still have these additional pharmacies that need to open. We're learning more as we-
Tim Pickett: And those still need to grow.
Rich Oborn: Right, yes.
Tim Pickett: There is a ways to go still, before full implementation and we're to full capacity, we've got a ways to go.
Rich Oborn: Right. But I feel like the legislature took some steps to set a firm foundation that we can build on, and we'll see where some of these amendments will lead us.
Tim Pickett: Yeah, okay. Well, I mean I'm excited again. I kind of am. Rich has got me a little excited-
Chris Holifield: You got to try these things.
Tim Pickett: I still think there wasn't any appetite for increasing patient caps this year. And hopefully next year, we can get around to that. That will be our big, hopefully, they can understand that I think it's okay to have a couple of medical cannabis specialists around town. But other than that, I like this provisional card thing I think is my favorite. There's some real benefits to having the 90 day renewal go away and just make that much more straightforward for people. So there are some things in there that I think are going to be good.
Chris Holifield: My only complaint is when are we going to be able to start bringing prices down? But I guess that's not up to you guys really. That's up to the pharmacies, I guess what they're charging.
Rich Oborn: I think there were some efforts to decrease the prices that the total cost of being a medical cannabis patient in Utah, one of those-
Chris Holifield: I'm talking before the medicine is selling.
Rich Oborn: Right, and I think if you take the big picture, and think about the total cost of being a medical cannabis patient, you can focus on the healthcare transparency tool.
Tim Pickett: And you you can also focus on increasing the number of pharmacies by making a 15th. That in general should decrease prices overall.
Rich Oborn: Right. So when you look at the prices of a beginning medical cannabis program, I emphasize medical cannabis, medical only. If you compare us to Arizona or to Colorado or to Nevada, you're comparing apples to oranges.
Tim Pickett: Yeah, because of rec, it’s completely different.
Rich Oborn: Right, but ours is a medical program. So if you compare us to the other medical only programs, we're in the middle and we just barely started. So you ain't seen nothing yet. That's kind of what I think about when I think about where we're at. A year has passed. It takes a while. It's like a big stone and gosh, it's slow at the first, right? Because it doesn't have momentum, there's a few little things that are rough, but it gets rolling, it gets rolling, it gets rolling.
Rich Oborn: And at the same time, we're protecting patients. We're protecting the public. Law enforcement becomes more aware of what's happening. I think the federal government, we're seeing more attention to medical cannabis and cannabis in general. But I think in Utah, for the foreseeable future, it's going to be medical only. Things get rolling. So I hate to remind people about this, but it's true that you just sometimes have to be patient with some of the realistic factors that are in place. We started moving a little bit quicker toward, I think true progress in our medical only program during the last session. When what we've talked about today actually begins to be implemented in 2021, that's when we'll be able to start to, I think, learn about the changes and see how this limited medical provider idea makes a difference, the controlled substance database.
Rich Oborn: Are they actually using that as a tool? Are people using the healthcare transparency tool? It just takes time for this big boulder to get moving more and more. But it will get, it's moving quicker than it was before.
Tim Pickett: Oh, yeah, I'm just grateful it's here, man.
Rich Oborn: Right. And we still have a goal of ensuring that patients get access under the supervision of a qualified medical provider and a pharmacist at a pharmacy that is more educated and is in the niche of medical cannabis and understands what products interact with what medications even better than we were when we started the program. So that's the goal of Utah's program. We want to make sure those connections between the patient and provider stay there, and we're moving forward and I'm excited about the base that we've created and building on that.
Chris Holifield: I'm excited too. Do you have other questions? I guess we covered them all on here.
Tim Pickett: I mean, really I'm sure I'll have questions for Rich tomorrow.
Chris Holifield: When people go to the EVS site, the EVS, what's the website?
Tim Pickett: Well, they have the government website is medicalcannabis.utah.gov, and that would have all of this information too or eventually I guess it would all be up.
Rich Oborn: It will, right. So again, the the governor still hasn't signed the bills we've talked about today. But that will happen I hear soon, we expect. And once those pass, we'll be able to update our website with some fact sheets and some information where people can go for some of the general high level information. And it's just important to keep in mind, these won't launch immediately. A lot of the changes we've talked about, it will take us some time. But yeah, they can find more information at medicalcannabis.utah.gov. And we see our numbers growing more and more and more providers are joining the program. That number continues to increase, which is really healthy for our young program to see the number of providers continue to grow. Also, something that changed I'll just stand with is that physician assistants no longer require-
Tim Pickett: We had a huge, huge win for PAs in Utah becoming essentially independent practitioners, but equivalent to the nurse practitioner, from an independent standpoint that after five years of practice, you do not need a supervising physician any longer in our role as PAs. It is a massive, massive win for PAs practicing. And having the ability now to be a QMP without a supervising physician, this QMP is just an added benefit to that. But it's a big deal.
Rich Oborn: Right. And so who knows? I mean, the cost of getting service could decrease because of that to actual medical cannabis patients because of that change because that PA doesn't have to have that supervising physician anymore. Because in the law, the former law, there was a requirement that that PA have a supervising physician who was also a qualified medical provider. So Tim operated like that, but in the future, he won't.
Tim Pickett: Yeah, I don't have to. Yeah, I mean I caution all providers, please get medical cannabis malpractice. It's really, really important before you go out and recommend any of this stuff and know what you're getting into. But if you've got questions about that, and you're a provider, you're a PA out there, then reach out to me at utahmarijuana.org. I talk to PAs almost every, a couple of PAs and a couple of NPs every week, help people get connected with medical malpractice if they need it. We have great contacts for that. I don't want to, I mean we can't take care of all the patients but we would definitely be able to take care of a lot, but we definitely need more people who are actively involved in this program. Well, thanks for coming out Rich. We're going to have, I'll put a fact sheet and a blog post together utahmarijuana.org and at utahmarijuana.org/podcast with this episode. Chris posts those episodes every week.
Chris Holifield: Every Friday.
Tim Pickett: Every Friday at 4:20 in the morning.
Chris Holifield: Every Friday, 4:20 comes in your podcast feed. So make sure you're subscribed.
Tim Pickett: And we'll put these legislative updates there. So you can come there and you can get a highlight of all of these things that might affect you as a patient. And I think that will be a good place for people to go get a synopsis before the state or race the state to get it up.
Chris Holifield: Well, thank you so much, go subscribe to the podcast, follow us on Instagram.
Tim Pickett: Stay safe out there, everybody.
This week's episode of Utah in the Weeds is unique in so many ways. It is a conversation between a farm-to-table grower by the name of Margie and your regular hosts, Tim and Chris. Margie's business partner, Natasha, interjected from time to time when her perspective as needed.
Long story short, Margie and Natasha are growers up in Cache Valley. [02:50] They run a very small operation which they have recently expanded to include a limited list of retail hemp products. They no longer deal with biomass given the significant drop in prices. Instead, Margie and Natasha are focusing on the retail market. [15:31]
Most of the conversation centered around all the problems Margie has gone through in her effort to get her products to market. [08:21] She explained to Tim and Chris how difficult it has been to find a bank willing to work with them. She has also had trouble finding a reliable e-commerce partner. In short, the first two years have been nothing short of challenging.
What makes their operation so different is their passion. [28:51] Margie and Natasha truly love growing. They must, because they both hold down full-time jobs apart from their farm. Margie said all the work is worth it when she sees a field full of mature crops.
In addition to the bank and merchant challenges, Margie has struggled to secure reliable shipping. [18:16] She even had trouble with the local community when she first began her operation. [44:47] Her willingness to keep at it is a testament to her belief in hemp as a product that consumers need.
This episode can feel like it's all over the place at times. Still, the conversation is well worth listening to if you want to know what life is like for Utah growers.
Chris Holifield: Let's get going here. This is episode 49 of Utah in the Weeds. My name is Chris Holifield.
Tim Pickett: And I'm Tim Pickett, medical cannabis expert here in Utah. I'm excited. This episode is a recording of a conversation we had with Margie from The Hemp Folk up in Cache Valley, Utah.
Chris Holifield: Such an awesome conversation. She shares some fun stories. Well, not fun stories, but funny stories that she had to deal with even in the postal system. Shipping hemp through the mail. We'll get into that in the conversation.
Tim Pickett: This is one of those really down home local interviews. Her stories are just classic troubles with the hemp and CBD industry. It seems like she's had them all. It's fun to get to know her.
Chris Holifield: And then the obstacles she run into with the city. But I don't want to give too many spoilers. We're going to get into that here in just a minute. But you have some news going on with utahmarijuana.org.
Tim Pickett: Yeah. Utahmarijuana.org. And our clinic side, Utah Therapeutic Health Center, has opened a location for medical cannabis evaluations right inside the same building as Wholesome Co cannabis pharmacy. We're inside the same building, that Carr building there in Bountiful. We have a separate space. We're not part of Wholesome, we have our separate space. So that's important to know. So this is a legal thing. I want to make sure that there's that separation. Chris, you and I are going to do either a short episode or some more information, detailed information, probably next Friday, I hope, or a couple of weeks from now, where we're going to go through some of the legal changes over the legislative session. There's been some pretty big updates including another retail license coming.
Chris Holifield: Yeah. I'm excited to hear about all those laws.
Tim Pickett: Yeah. And changing to the way people get their cards, hopefully a little sooner instead of having to wait for the state. So we'll give all those updates in an upcoming episode.
Chris Holifield: Very cool. And then people can go check out the podcast you utahmarijuana.org/podcast. Go listen to them there, and make sure you're subscribed in whatever podcast outlet you're in ... that you listen to podcasts in. Obviously, the podcasts are free to listen to. So go check them out, go consume some great content about the cannabis community here in Utah. So anything else you want mention, Tim, or should we jump into this conversation with Margie?
Tim Pickett: No. Let's jump in.
Chris Holifield: All right. Here's that conversation that we have with Margie from The Hemp Folk. Thank you so much for listening. Enjoy the conversation.
---
Chris Holifield: How long have you been hemp farming?
Margie: So we started right when Utah allowed hemp farmers to grow. That's in the 2019. So 2018 we applied for growers permits, we got them. We've been farming for two years now in Utah.
Tim Pickett: Yeah. And your farm is up in Cache Valley. How is that because it seems like that's not the ideal climate for cannabis?
Margie: Well, I think that it will depend on the strain that you're growing. But the strain that we grow was the hope and express mostly. We also grew a bunch of other strains the first year that we got from Boulder Seed. There were some that were better suited for the climate than others. We grew a lot. We grew about three acres that first year outdoors and there was one strain, San Cinco, that turned out awesome in the beginning, and it grew super big, and it was great. And then two windstorm happened right when they were almost mature and knocked maybe a quarter of them down. There was so many things that we learned along the way. Both years have brought-
Natasha: Something new.
Margie: ... something new. Yeah.
Tim Pickett: You're learning something new. Did you have a lot of background in hemp farming? Tell us a little bit about your background because that's really interesting.
Margie: My background. So there's two of us. I am Margie Borecki, and we also have Natasha Quinones-Rodriguez. And I have a background in landscape architecture and environmental engineering, where I studied plant uptake of nutrients and metals. So I got a doctorate in how plants are ... the amount of nutrients and metals that various plants in stormwater detention basins took up. We speculate on the reasons as to why different plants work better, where the nutrients and the metals go. Whether it's in the soils, in the water, in the poor water, or in the plants, and what part of the plant? So if you wanted to look up my dissertations, those are super very thrilling and I bet you would like them, but not right at all.
Margie: Natasha on the other hand has a horticulture degree from Puerto Rico. She was the day-to-day person who really made a lot of the decision making when it came to, "Why's this plant yellow?" And Natasha would be like, "Well, I believe that, and we need this." And I'd be like, "Okay. Yeah. That's great." Because even though I have a degree in the uptake of nutrients and minerals in plants, my degree is not in how to keep plants alive, it's in what happens. So Natasha worked a lot with the plants and together, we were great checks and balance system. When I'm watering, I would be like one, two, three, four, next. One, two. And Natasha would like, "This one needs more." Back and forth I'm like, "Why did you do that?" And I'd be very meticulous, and she'd be like, "That one needs a little extra love of some kind." So we would go back and forth between the two of us. Whatever we did worked, it worked.
Margie: We had quite a few people in the valley here. I don't want to name names. I guess maybe I can, but somebody from UDF who would come up. So I just won't name a name. And they said, "Wow, this is one of the best grows." As far as the plants themselves that they've seen in all of Northern Utah, and it was true. We have a video up on our website. If you wanted to see it down at the bottom where we had a little bit of drone footage in an interview with me. A friend of mine had done the video. I like looking at the video just to remind myself how beautiful it was.
Chris Holifield: I watched that video a couple weeks back and I couldn't find ... What website is out on is that on? Is that on the intentionalfolk.com website? Because I'm not seeing it on there.
Margie: All the way down at the bottom is a video. It used to be thehempfolk.com, and it should now. So we have issues with the website. So we're rebranding. We have a farm that's called Intentional Growth farm, and we have products that are called The Hemp Folk products, right?
Tim Pickett: Yeah. Those are what I've seen online, right?
Margie: Yeah. And so this is still going to happen in the next couple days. We're rebranding as Intentional Folk because we might have, one, merge the two together so that people know that the farm and the products are the same, but two ... The products will still be called The Hemp Folk products, but two, because we don't have an e-merchant that will work with us. So we have e-merchant issues which are very separate than the farm, but we have e-merchant issues. The financial system has been very challenging for us so far.
Tim Pickett: Yeah. It's that hemp CBD transacting, right? It's selling CBD products online and finding a merchant or a processor that will work with you. Is that really the big problem?
Margie: Changing topics quite a bit, but originally, I had a bank account as a farm and that was fine. It was from a local credit union that I have five other bank accounts with. And one day just out of the blue, they're like, "You're a marijuana related industry. We no longer want to work with you. You have 30 days to get a new account."
Tim Pickett: Wow!
Margie: Yeah. And so I was like, "Well, crap." So I called a bunch of other banks that are hemp and cannabis friendly banks. Three of them told me I'm much too small that they're not even going to touch me. One of them said yes. And so I did all the paperwork and I waited probably two or three months. They came back to tell me that because I'm planning on selling more than 10% ingestibles on my website, they can't work with me. I would be paying for them to check my bank account every month, right? And I cannot sell more than 10% profit from ingestibles because of the different state laws. And so I'm without a bank for months. I finally found a bank in a different city in Utah, and they say, "We do business with hemp farmers in Utah, in Colorado, and Idaho, and I'm like, "Thank God." And they're like, "Yes, of course." And I gave them all my information and they're like, "You're out of our jurisdiction." I'm like, "I'm in Utah." They're like, "Yeah, but you're not in our part of Utah." Again I'm so upset.
Margie: I have a person on my LLC simply because they live near a different thing that really was willing to work with us. They are a member of our LLC simply because I needed a bank account and that bank was willing to work with us, and I needed to live within their jurisdiction, and it was a different… Yeah. So that was huge. That was one hurdle as far as financial institutions go. Another hurdle then was the e-merchant. The website itself, the platform that you're doing your website on has to be marijuana and CBD friendly. For example, wordpress.com is not CBD friendly. WordPress.org is free and it is CBD friendly. But my website designer is like, "Let's go to Wix. They're CBD friendly." I'm like, "Okay. Great. Let's do it." So we do it. And Square works with Wix, and Square is CBD friendly. Everywhere you go, it says, "CBD friendly, CBD friendly." Except they ask me for information and I gave them the information.
Margie: The next day, they asked me for the same exact email. "So you still need to provide us with information." So I gave them more right because they asked for different types of permits and business registrations. So I gave them more. Third day, they asked me for the same thing, exact same email from [email protected]. And so I'm like, "What am I not doing? Why are they not getting my information?" On my website it also says, "Make sure that there's no medical claims on your website." I'm like, "There's no medical claims on my website." We scour, we take just stuff off because we want to make sure there's no medical claims. A month later, they're like, "We're sorry, you're disqualified." For that month, I think I wrote 20 or 30 emails to [email protected]. I did live chats. "Type in what your problem is and we'll get someone to email you." Nobody calls you, nobody talks to you. They have a phone number, the phone number says, "I'm sorry. We're not taking customer service. We're just not taking telephone numbers." Even though they have a phone number, I couldn't get a single human to talk to me.
Tim Pickett: Wow.
Chris Holifield: That's crazy.
Tim Pickett: That's really crazy. Of that experience, now do you feel like you're solving that issue or is it becoming easier for you?
Margie: I don't know how much I can tell you without getting myself in trouble how I'm navigating this because I've talked to different e-merchants. And the problem with other e-merchants that I've had in the past, one, you pay 30 something dollars a month simply to have them, two, if there's ... Instead of having a 4% fee, it's six, or seven, or 8%. Of course there's a fee on top of that. Then the two that I've talked to both of them had a $40,000 minimum of sales you had to produce that month in order not to have an additional $300 fee. And I was like, "Wait, what? There's no way I can ever have that. I don't even know if I'll have $300 every month. I would hope but I don't know this." I don't have $300 to give them every month. We're day-to-day here. And so it's been challenging.
Margie: We thought that after our first year of growing, I remember telling Natasha and Natasha reminded me. I'm like, "I took out the loans, I took out all of the financial risk. I took the financial risk in the situation. And I said to her, I'm like, "If we are struggling to pay labor because our crop is so beautiful, and big, and wonderful, at harvest, we have done something right and that's where we want to be." So that first year we do everything we can. We are struggling to find labor, we are struggling to keep up, we are finding storage locations because we can't believe how much crop we have. We had somebody who just came in and they just ... they did half of the field for us because it just was so overwhelming for us. Even though we were there every day, it didn't click how much vegetation that was. And I'm like, "Fantastic. We have this amazing crop, we have this amazing biomass, we have these amazing flower because we started to dry, to cure the flower." And now I'm like, "I don't know how to sell it, and I can't sell it."
Margie: What used to be $30 a pound for the biomass, is now six. And I'm like, "Wait, so what you're telling me is if I sell this to you, I have to go bankrupt. Okay, I can't do that. I just can't do that." I can't pay off my debts. So how do you go about this? Which is why we started The Hemp Folk and The Hemp Folk products. It was within a month. We're like, "Okay. What do we know?" We know that hemp, the flower isn't selling. We know that there are processors and we know people are still buying. The buying hasn't stopped. So we quickly we ... What would it be called? The go-to phrase during the beginning of COVID. You need to pivot. Well we pivoted long before COVID started. We were like, "Oh." So we did anything and everything we could to try to stay afloat. We both have full-time jobs this year. And then we still have a farm, we still have a warehouse, we still have the product, we still sell everything. Everything is still going on. It's just more intense.
Chris Holifield: More hurdles to jump over, it sounds like.
Tim Pickett: Yeah. It sounds like you're still dealing with the banking and e-commerce type stuff. And hopefully that really gets better. You're threading this needle with the financial system, but at the same time you dealt with ... You talked about the crash in hemp prices, right?
Margie: Yeah.
Tim Pickett: From $30 to $6. And we've talked to multiple people about that. When we talked to Kyle Egbert, he described that too, a clean leaf and just the fact is the biomass market just tanked.
Margie: Just crashed.
Tim Pickett: Right. It just crashed.
Chris Holifield: Remind me what caused that, Tim. Did we talk about that? Why did the biomass market crash? What was the reason?
Margie: In 2018, Utah allowed for hemp to be sold ... to be grown via the 2014 Farm Bill, right?
Chris Holifield: That's right.
Margie: But it's a 2018 also passed the Farm Bill. So other states automatically allowed him to grow. So all of a sudden we're going from ... the numbers are off, but from a handful of states growing hemp to 20s, 30s states that are growing hemp. Thousands, thousands, and thousands of acres of hemp. Everybody had the price data, $30 per pound. I would have been sitting much prettier than I am right now and everybody else would have. They were so much-
Tim Pickett: There just was so much biomass because all of the farmers who just decided, "You know what? This is going to be a great opportunity. Prices are 30 bucks, we're just going to grow hemp." But then everybody kind of ran into the same problem you did, right?
Margie: Yeah. Who we're selling to.
Tim Pickett: Yeah. Who are you going to sell it to? And so the market just crashes. Interesting.
Chris Holifield: Who was the plan to sell it to before you even started farming though? Was there a plan in place there of how that would work there?
Margie: So there were the processors who would have bought it if they weren't inundated. But because they were inundated, they started doing the 50/50 contracts or something along those lines. They were like, "We don't want to do the 50/50 contracts. We're only want to sell it for six, seven dollars a pound." And at that point, you're like, "Okay. Well then, who else wants to sell it ... to buy it?" I can sell my flower. It's cured, and it's beautiful, it's smokable, but who can legally buy it? And that was a lot. Trying to mail hemp that first year was intense. I got good stories about mailing hemp as well. There's been a lot of good stories.
Chris Holifield: Let's hear one of your good stories about mailing hemp before we forget.
Tim Pickett: So this is you selling smokable hemp flower to somebody in another state because you can't sell it in Utah.
Margie: Can't sell it in Utah, can’t sell it across state lines, though it's totally legal.
Tim Pickett: Well, okay, yes. But it smells like weed.
Margie: It smells like weed. FedEx may or may not be send it someplace, UPS may or may not. They both have policies in place saying they will not send hemp. But they haven't fixed the policy to say yes, we will. I guess it was more accurate. The post office has a policy in place. We will. It is federally legal, we are a federal entity, hemp is legal. All right. So I think the first time something happened with the mail is that I'm sending it to a lab in Nevada to get tested to see what we have. Once it's been cured, it's been harvested, cured, we want it tested. Nothing's coming back and I'm like, "I need this because I need to be able to sell it." I don't know what I'm going to say. I don't know about the CBD percentage, I don't know if it passes all of the requirements. And a week later, nothing. Two weeks later, they're like, "We don't have anything." And I'm like, "Whatever." So I called the post office. And I think I had kept track of it that time.
Margie: I think I spent 10 hours on the post office phone waiting for people to answer. Once people answered, they told me there's not much they could do, blah, blah, blah. Finally, it got to a place I get a letter in the mail saying, "Call this number." And so I call the number and the lovely lady is like, "Okay, so that's what you think? Okay. Somebody will call you back. And I was like, "Uh-huh." So now it's been another week, somebody does call me back and they say, "Oh, it's industrial hemp. Can we open it up?" I'm like, "Yeah. Go for it." It's industrial hemp, all of the information is in there, our grow permit is in there, everything is in there.
Margie: Okay. Now, mind you, on the tracking of the package, it said no such number. It said that I put the address in wrong, it didn't say picked up by the postal inspectors, which is very ironic because I actually work for the post office now. I think it's pretty cool that I get a job at the post office and I'm like, "All right. People should tell me all these things." I've even met some of the postal inspectors that have inspected my packages which is also very cool, almost by accident. How cool is that, right?
Chris Holifield: That's awesome.
Margie: Now I get to ask them about stuff all the time. But so this is now three weeks since I originally sent the package. I sent a different package via FedEx probably illegally, but I'm like, "I need to try something else because I need the results." And so that already comes, I already got my results, and now the original package finally it gets to the lab. We have issues because they think I'm wanting to get that analyzed again, and they charge me again, and I'm like, "Wait, no." There's just all these things that are constantly happening, all these little roadblocks, but they finally get it. The second time this happens, we send it to a smoke shop somewhere in the Oregon Washington coast and it's similar. And now this time the person who ends up calling me back I don't freak out because for a while I was like, "Are they going to come to my house knock down my door? I don't know." You just don't know what's going to happen. Everything was so new at the time.
Margie: The second time, I get a person on the phone and he was lovely. He tells me people on the post office line, they don't see a package, smell it. They don't know what the difference between marijuana and hemp is. And I'm like, "But I'm the boss. It says certified industrial hemp." He goes, "They're thinking it's marijuana. They put it here. But yes, you have every right to send it." I'm like, "But now it's four days later. The hemp might have been sitting in the sun the whole time and gotten mold." I don't know. And he's like, "Well, do you know what we can do? We can put you on the vetted list. So I'm on the postal vetted list, which is a good thing. Everybody should be on the postal vetted list. I have no idea how to get on this vetted list. All I know is he sent me an email, I sent him back information, I got on the list.
Tim Pickett: ow!
Chris Holifield: That's cool. Yeah. So basically your packages won't get messed with anymore.
Margie: No, they still do because I sent 100 pounds, six different packages, 30 pounds each.
Chris Holifield: Oh, my gosh.
Margie: This is a $25,000 load ... package that I'm shipping to California. And I had a signature confirmation, all of the things and it gets stopped. And I'm like, "Well, crap." So I finally call the postal inspectors and I'm like, "Listen, I'm on the vetted list. Just talk to me." They find five out of the six boxes. They're like, "Okay. They're sitting over here." But it's been four, or five, six days. By the time they get it, it's a week. The people who get it they happen to get ... they're a marijuana dispensary, that they're buying from me. They happened to have gotten robbed at gunpoint or something. So they're busy. By the time I call them, they tell me that all of my stuff is moldy.
Tim Pickett: Oh, wow.
Margie: $25,000.
Chris Holifield: Just down there. So you lost it.
Margie: I lost it.
Chris Holifield: Oh, my gosh.
Tim Pickett: This is crazy. What are you supposed to do? Just drive it yourself?
Margie: That's your best bet.
Tim Pickett: For $25,000, I'll drive to California too. You can sign me up, I'll start delivering for you.
Margie: I wouldn't be able to pay you the whole thing, Tim.
Tim Pickett: No. Of course not. That is pretty interesting that you can still get on the vetted list.
Margie: Even on the vetted list. They had no problems with it. It's just that it had to go through the process.
Chris Holifield: You can't mail it to customers. It just seems it gets lost, they take it, it gives you a bad name to these customers because these people aren't understanding why they're not getting it because they're like, "Well, it's legal. Hemp is legal. Why can I get it delivered in the mail?" That's crazy. I just can't believe it. So what needs to be done to stop it? I guess just full legalization of everything is really the only way to stop that. What do you think the way around that one is?
Margie: Our process now is that when we send it, one, absolutely 100% it's not only in a smell proof container, locked container, it is in three baggies, three separate baggies, three different sizes. There cannot be smell because as soon as there's a smell of any kind, people love catching this. They love catching it. It's a game.
Chris Holifield: They feel like they were a hero. They're like, " Oh, yeah."
Margie: Yeah. At one point I had on the top of the boxes, I said, "I am on the USPS vetted list. This is industrial hemp. Please call this number if you need anything." They still stop one of those packages. It just had to go through the due process because just what if she's going... Maybe if the post office offers, you would have to always go through your ... Whether it's Click-N-Ship, or Shippo, or Shopify, you would have to have a designation when you print your labels and pay for your labels to yes, I am a vetted industrial hemp farm. Up for now, that hasn't happened, that doesn't happen. Who knows.
Chris Holifield: And I would imagine all hemp farmers are running into this. Obviously it's everywhere.
Tim Pickett: This seems like it's a crazy system problem. It's interesting because on the other side, there seems to be so much CBD out there right now, right? And there's so many products good, bad, your products are good vetted products locally. You're like farm-to-table, CBD, right? That's the whole idea.
Margie: It really is.
Tim Pickett: Cache Valley cheese, Cache Valley hemp.
Margie: Well, not only is it farm-to-table. The process that we use is a traditional extraction process. Some of our products do have distillate in it, but most of our products in a large majority of the CBD comes from traditionally extracted methods. It's not even going through alcohol or through a CO2 extraction process.
Tim Pickett: So talk to us a little bit about that traditional extraction methods, when you make your oil or when you make your gummies.
Margie: So for the people who have done it themselves think cannabutter, but we use coconut oil. I've worked in a lab for seven years right getting my PhD, that's what I did. I did lab research and field research. With the coefficient to account for loss, I knew how to calculate. If I put in this much hemp flower in the hemp flower has this much percent CBD with a coefficient of probably 80 to 85% if it is going to stay in the oil, how much CBD am I going to have in the oil? And when I did the calculation the first time and then we had the certificate of analysis for the coconut oil, I was stunned how close I was. I was like, "Holy crap. We could do this over and over again." And so we just have to make sure that this happens with a process like in working with a processor.
Margie: I've been fortunate that I was friends with two different processors and I get to work with them at their place under their license to get this done. I just do it for myself. Because I use my plants, we only use the flower that's been trimmed and because that way I know exactly what I'm putting into the oil. If I was to put biomass in it, it wouldn't be concentrated enough.
Chris Holifield: Interesting.
Tim Pickett: That's interesting. I really like this idea. This is the classic farmers market hemp to me. This is what it sounds like to me. This is not an industrial processed farm, this is a small farm. Do you want to grow bigger, do you want to do more, or do you want to just stay farm-to-table?
Margie: Do we want to go bigger, do we want to grow more, or do we want to stay farm-to-table? I asked Natasha because Natasha loves to grow. There is nothing more beautiful than being especially towards the end of August September October, the very beginning. October becomes a little too busy. So I guess September is this beautiful time. There's nothing more beautiful. I would stay at the farm 24 hours a day. There's nothing more lovely than being there, being inundated with the beautiful smell in the ... You know that this plant is a good plant. It just brings so much happiness. Everybody who comes there is like, "It's so nice." I'm like, "Yeah. So nice, and so beautiful, and the plants are beautiful." We had a herd of rodeo horses run through while the big plants were still babies so everything's turned out fine. It was really, really cool. It's so beautiful. I would love that. And Natasha if she could, that's all she would do. She would stay out at the farm, she would not do any of this other stuff. But we have to do what we have to do.
Chris Holifield: How big is your farm now? Do we even talk about how many plants or how many acres your farm is now?
Margie: So originally in 2019, the farm was 3,800 plants or so. Something under 4000 plants. And again, we could not physically harvest. Because we did it all by hand, we could not physically harvest half of it. So somebody else ... they ended up taking our plants from us. In theory, we're splitting the profits, but we haven't seen anything from that yet. It's okay. It's only worked out fine. Last year, we went smaller. How many plants did we have last year?
Natasha: 2,000.
Margie: 2,000?
Natasha: Mm-hmm (affirmative).
Margie: We had about 2,000 plants last year. And that was much more doable. And we focus this year not on biomass. There's no reason for us to do biomass at this point. So we focused on getting the flower. Because it grows outside, everybody should worry about plants grown outside, any plants. When you get it tested for the microbial populations, outside plants will very often have aspergillus. I mean, every carrier will have that, everything will have that, but if you're on a farm, it's very likely you'll have aspergillus. And so some of our flowers last year that was outside flower because, we also have a greenhouse, some of the outside flowers had aspergillus. So in order to combat that, what we've done is we actually wash the plants. Right after harvest, we actually take every single physical plant, dip it into a hydrogen peroxide solution, dip it into a water solution, dip it into a water solution, dip it into a water solutions, then hang it up to dry. That kills all of the aspergillus so that we know and I can feel super comfortable being like, "You could smoke this, you can eat this, you could do whatever you want, everything." Now imagine doing all that and still not having anyone to sell to. You lose hope that this is ever going to work. It was so much work and it was a lot of fun. Truly, we have so much fun.
Margie: We have a group of people here that are 18, maybe 19 is the youngest that we have, to a woman who's in her 60s who comes and helps all the time just because everybody just loves hanging out. This is fun. This is a fun great thing to do and you feel you're a part of something. That's probably why we're still doing it again. So this year we grew the 2,000 plants. We only focused on the flowers so that we had much less shared space that we needed to have ... to dry and we just focusing on curing them.
Chris Holifield: Margie, I was reading somewhere on your website a couple weeks ago, when we were originally going to talk to you, that you guys you grow edible mushrooms too there on the farm or something like that, or you did?
Margie: We still do under our umbrella. Natasha is here, but we don't have to headphones so I'm going back and forth with her.
Chris Holifield: Sure.
Margie: We actually also grow edible mushrooms. All right. Tell me the names because I've forgotten.
Natasha: Pink oyster, king oyster.
Margie: There are different types of oysters. There's the pink, the king oyster, we have the shiitake, we have lion's mane. So it's the same farm, it's just at a different location. This one is on a residential property, but we have a greenhouse that we grow them in and do all of the sterilization, and that's necessary for growers.
Natasha: We grow them in hemp stocks.
Margie: What was that?
Natasha: We grow them in hemp stocks.
Margie: So one of the reasons we did that is because we had all these hemp stocks. And we're like, "What are you going to do with this?" If you burn it, it smells like weed and then the whole, all of Cache County, the sheriff department is going to come. So we don't want to burn it. And well, and we could always compost it but we're like, "What can we do with this?" So we grow them on hemp stocks.
Chris Holifield: Interesting.
Margie: We put the mushroom on the ... What's it called?
Chris Holifield: We inoculate.
Margie: We inoculate them in the hemp stocks.
Tim Pickett: This is cool. And then what do you do with those? Do you sell those? Do you just eat them up?
Margie: Both. Mushrooms are so good. We try to sell them. For now as long as we're as we were going to have a market here in Logan that we were going to do mushroom Mondays, but we didn't have enough interest. So we were trying to finish the mushroom greenhouse. So we're doing all of the things at once. It went back and forth and we did what we could when we could. For right now, it just was cold.
Margie: So we just decided that we had to build another shed so that we didn't have to do the sterilization inside of a small kitchen. We built a shed so that we can have the sterilization done there. And that way that's right next to the mushroom greenhouse, and then it'd be an easier back and forth instead of trying to get it all. Because you have to have it all sterile. And so we have these 20 gallon totes that we have little holes in and you have to put in your hands inside of the gloves, and then you work with it and try to inoculate the hemp stocks. Because as soon as you get any bacteria in there, the bacteria will overtake it.
Tim Pickett: Oh, wow.
Margie: It's an interesting process. It's all Natasha. I would love to be able to take the credit for this, but truly, it's all Natasha. I know how I've been helping, all of the things but truly this was a Natasha brainstorm idea that she's like, "I just want to try it. I want to learn how." And she's been all over it since then.
Tim Pickett: Yeah. It's super cool. And I think that they go together honestly.
Margie: You got to be ready for the future.
Tim Pickett: And that's really the point. You need to learn how to grow these things because the research around mushrooms is it's going to come fast.
Chris Holifield: Mushrooms are good.
Tim Pickett: Yeah. Like psychedelics come as far as from a medicine standpoint. I've been doing myself a lot of research on addictions and resetting the narrative for people. We'll talk more about that when that comes down the road.
Margie: The potential is just huge. I'm really hoping that the narrative that ... just the everyday narrative around the United States changes. And it has been starting to change, which is a positive, right? We all want that, but maybe not all of us. All of us that are not scared of it want it.
Tim Pickett: Yeah.
Margie: We have to have something else rather than chemical pharmaceuticals that truly there has to be something.
Tim Pickett: So go back to this uptake of nutrition and uptake of this. All of this stuff that gets put into this plant. How does your education really adjust what you're doing for these plants? Can you manipulate what they're what they're taking in? It seems like you could.
Margie: Actually I could, but I haven't. What I know how to do right now is to document what we have been doing. I'm not in a position where I could be like, "You know what? This week I'm going to focus on something that I don't have to do to make food readily available on my table." Because it does take brainpower and it takes physical time to try to get these things done. And I don't have the access to a laboratory to take more tests. I think what the benefits of my education truly are is that I am so completely process driven.
Margie: I don't do things because I think it's a good idea, I do things because, wait, if I do point A, it should give me the point B, and once we get to point B, we see that it's either going to go C or D. And if Because see, this is what we should do, and if it goes D, this is what we should do. That's why Natasha and I work so well together because I'm like, "Wait, wait, wait, wait, wait. We're not at sea. You can't keep doing that." And so we go back and forth. Were constantly assessing and positioning ourselves to try to get the best results. That said, I think that what we've run into last year, so 2020 was just time in energy roadblocks. And I think that those were probably two of our largest roadblocks. We didn't have the time to do all the things we wanted to do. And we sure didn't have the energy to do all the things we wanted to do.
Margie: With that, we don't have the money to pay someone to do those things either. We did the best we could knowing that somethings had to give. In agriculture oftentimes something has to give. I think any farmer will tell you that's obvious. That's not an option to try to do all the things you want to do. It's a matter of what you can do.
Tim Pickett: This is an inspiring story, I feel like. I really love this.
Margie: Thanks.
Chris Holifield: So It looks like people can buy your products right on your website too, on the intentionalfolk.com or Hemp Folk website, right?
Margie: That's correct. In the state of Utah, I have a retail license and we can sell any product, any of our five products in the state of Utah. So we have gummies tinctures, body butter, and topical oil, and lip balm. But online, I can sell anything just about anybody. You have to know what it is legal in your state, and the burden is at that point on the buyer, not on the producer.
Tim Pickett: Right. But in Utah, you can sell all of this stuff and you have your CRAs right there online.
Margie: Mm-hmm (affirmative). Yes. They're all there. So at those five products absolutely. And now that the bill passed, so we can start selling hemp flower in the state of Utah. It just has to be registered with the state and you have CRAs for it postharvest, not the preharvest that the state does for you.
Tim Pickett: Got it. Not the stuff that says, "Okay. This is not hot. This has less than 0.3% THC."
Margie: Yes. It cannot be that one.
Tim Pickett: But now you can start selling smokable flower to a consumer.
Margie: As long as it is labeled, as long as it's clearly states that it's ... which I think is strange. That is for medical purposes only, and it does not look like candy, not for anyone under 21, and it has to have point 0.3% total THC or less. Even though it's that's the law for hot, you can't sell it also.
Tim Pickett: I see.
Margie: If it's above the 0.3, even after harvest and after curing.
Chris Holifield: And if you're lucky if the post office doesn't catch it and hold on it.
Tim Pickett: And hold on to it.
Chris Holifield: Especially in Utah, you're mailing within the state.
Margie: Okay. It really is. It's kind of a dog chasing after a squirrel or something. They're like, "It smells!" People just get excited.
Tim Pickett: They do. Okay. So theoretically, I can go to the farmers market next summer and I could buy smokable craft grade hemp.
Margie: Oh, I don't know about that. Theoretically, maybe. Yeah.
Tim Pickett: I think your problem is going to be testing.
Margie: Oh, okay. So I don't think that's actually accurate. I think in the bill it does say that it cannot be for smoking, it can be for vaping.
Tim Pickett: Oh, yeah. Okay. No flames.
Chris Holifield: Well, yeah. When I think of smoking, I just think of vaping.
Tim Pickett: To be honest, that's what I think about.
Margie: Me too. Yeah.
Tim Pickett: Yes.
Chris Holifield: That's awesome.
Tim Pickett: But this is a pretty big deal.
Chris Holifield: I hope somebody does that at a farmers market. I hope somebody's pushing for the downtown Salt Lake or Park Silly.
Margie: I don't think it'll be in Logan. I do not. Last summer I asked to sell my CBD products that are 100% legal, registered in the state of Utah. All of the paperwork, all of the registrations, they didn't want it.
Tim Pickett: Oh, wow.
Margie: And I'm like, "I grow it here, I produce it here."
Tim Pickett: You're the reason they're farming in Cache Valley. The whole point up there. Utah state is one of the world's top horticulture education centers, right?
Margie: The school of agriculture is world renowned. But there's still stigma, and dealing with that stigma is just ... So I will say this. I don't know if the stigma changed or if I've changed. The first year before this all ... Do we have enough time for one more really-
Tim Pickett: Yes.
Chris Holifield: I got all the time. Go ahead.
Margie: You could edit half of this out, more than half. You can edit most of this out. It is March, it's still snowing outside. I'm having a backtrack a little bit. I was working for a federally funded grant program for sustainable ad. I won't say where. It's easy to find where I worked, but I'm not going to say. And I told the farmer friends of mine, good friends of mine, "This is happening. You guys, you have to grow hemp." And they're like, "Margie, we're so stinking busy. We can't do one more thing." And I'm like, "Come on, please. Go ahead. This is the coolest thing in the world. It's dream come true." And they're like, "That's why we're giving you land to grow hemp." I'm like, "What?" They're like, "You do it." And I was like, "Okay." So that's how I started to grow hemp.
Natasha: A big shout out to them.
Margie: And a big shout out to Mt. Naomi Farms up in Cache Valley. If you guys ever have an event that needs to happen, this is so beautiful. There's super high class barn, and a real working dairy with a real vineyard. Unbelievable. These people are so, so amazing. But they also grow alfalfa. They wanted to gift me and lease to me, for a very reasonable price, three acres of land and helped me out all year long for the last two years.
Margie: And so I'm driving by, it's March and I'm telling a friend of mine. "Hey, friend. My farm is going to be right around here somewhere, right?" And I'm all excited. It's 7:00, 8:00, 9:00PM, it's dark outside, and someone's in front of me going pretty fast, someone's behind me also going fast. I'm like, "Oh, it's going too fast. I don't know where I'm at." It's the middle of the night. I've only been there maybe five times and I've taken the back roads. And so I'm like, "I'm just going to pull over, check my GPS. Okay, cool." I pull over, check my GPS. The car behind me isn't going forward. And so I rolled up and when I'm like, "Just go, just go," it's a state trooper, it's a sheriff. I'm a smart person, but I get really stupid when I'm nervous. I talk a lot, I tell everybody everything. "Of course, everything is good, everything is good. I'm going to be a hemp farmer." I'm going to have all of the wrong things come out of my mouth. Anything that I shouldn't have said, I said to the sheriff.
Margie: Turns out Sheriff lives in that neighborhood. Sheriff knows that there's adopted kids, foster kids. When they start selling hemp as marijuana at the high school, whose fault is that going to be? And we don't want no outsiders in our backyard selling, growing this bad stuff. And it was really interesting because this is a sheriff. And he obviously knows so much, but all wrong. Just twisted enough where I'm like, "That's not true. So many of the things you said are correct, but that's not true." And so it was really, really interesting how that type of information is so dangerous. Now, mind you, I had no way of defending myself. I'm like, "I'm so sorry. Should I write a letter? Should I tell everybody?" I was just completely and utterly not at my best at that moment. And my friend just was shocked. I didn't know how to stop myself.
Margie: So fast forward, I tell the people, the owners of the forum that this happened. They're like, "Did we ask them if the subdivision could come in?" "No." "This is legal. This is my land, you're fine." I was like, "Okay. I got to buy a gun." All right. I don't know what's going to happen. I do not know what's going to happen. A month later, I get a phone call from some folks that I happen to know also in the industry. One of them who lives in that neighborhood asks me, "Did you get stopped by a cop the other ... like a week or two ago?" And I'm like, "How the hell would you know? How would you possibly know that this happened?" He goes, "We had a neighborhood meeting. He brought you up, about how some outsider girl is going to come in and she's going to ruin our neighborhood." And I'm like, "Oh, my God."
Tim Pickett: Wow!
Chris Holifield: That's horrible.
Tim Pickett: Wow. So have they been somewhat more receptive?
Margie: No. They've been lovely. I'm scared. Don't get me wrong. I'm scared. I had hunters who would normally come and hunt on that land with their gun, with their rifles and I have my cameras up. And I'm like, "Oh, my God." Everybody's been kind, everybody's been nice.
Tim Pickett: That's good.
Margie: But the fear was huge. We got concealed weapons permits. You can't put on the actual podcast that we actually don't have any weapons, but we could.
Tim Pickett: That is awesome.
Chris Holifield: I'm so glad that you came on the podcast. You got some great stories.
Margie: And I'm sure that there's more. Truly, this has been such a crazy amazing experience. To your question, Tim, I don't know how I'm going to put this together with my dissertation research. There's a million ways. I was asked to give a bunch of information to the university and I'm like, "I could, but then what will I have?"
Tim Pickett: Yeah. It seems to me like you have done something that you set out to do. You've done your own research in a small way. A lot of people are talking about industrial hemp, and biomass and the extraction processes. We've talked to quite a few people in this hemp space and everybody has such a different perspective on it. And your perspective is really truly from this local ... the local farmer perspective, what do you do? How do you go out there? What are the hurdles? And people need to hear that because this is ... It's coming back, it will get easier, but the process of getting to the point where it's easy to where you can go down to the farmers market and you can buy some hemp flower, or you can buy some CBD body butter that was made in your town with natural extraction methods, the process to get us to that point is so ridiculous. That's the real story that I think people need to understand.
Tim Pickett: It's not just learning how to be a farmer and grow tomatoes, and you take the best tomatoes down and sell them. It's the sheriff, it's the permits, it's the weather, the rodeo ponies, it's dipping it in hydrogen peroxide and then water so that it's safe. It's the testing, all of that testing.
Margie: There's a lot of testing. Every time you have a product that is registered in the state of Utah, someone's paid $1,000 because between the CLA ... Mind you, I have a tincture that's a one ounce. In order to test it, it's 1,000 ... Well, it's $600 plus 300. I think it's $20 for the registration. Now, I changed that to make it strawberry flavored. I have to go through $1,000 again.
Chris Holifield: That's crazy.
Margie: I changed it just to make a different size. It's $1,000 again. That's why I have five products. I could do all sorts of great products and they're coming. It's a matter of making sure that I have that. What I tells Natasha all the time and anyone who's listening out there in podcast world, is what I need is an investor who's got about $100,000 that knows high risk commodity marketing because this is considered a high risk commodity. And if someone has high risk ways of knowing how to sell this, I'll be interested because I don't need an investor that knows how to grow, I don't need an investor who knows how to do any of these other things. I at this point need to figure out how to manage the realm of being able to get this out of the market because you can't do Google ads, you can't do Instagram ads, and Facebook will take you down.
Margie: If you're selling blankets, it's easy. Within a couple minutes, you set up your website, you get your Facebook people out there, you buy one of those ad things where you get a couple extra 1,000 followers and you're on your way. Oh, no. It's not nearly that. You just can't do it. And if you try to do it, they'll take you down because then you're hemp. So I'm like, "Okay." So you play this game. Okay. I'm on Instagram. I sell CBD products, but definitely not on Instagram. Instagram is just about how lovely my life is. And you play this game. I would love to be able to put an ad on there, but I can't. I would love to be able to say, "Buy my products." But it can. It's interesting.
Tim Pickett: I know it will get better. And you really are doing all the right things. This is really cool. It's cool to meet you and hear your story. You guys are awesome.
Chris Holifield: Margie, anything you want to add before we wrap this episode up? Any final words, or comments, or something that we didn't cover in this conversation that you were hoping we did cover?
Margie: So the easiest way to get ahold of me is email, phone, or website. Just the average, the normal avenues. I text so if you want to get ahold of me, 764-6666. 435 is area code. So 435-764-6666. Email address is thehempfolk.com. No. Thehempfolk@[email protected].
Tim Pickett: Thehempfolk@[email protected]. And that is on your website, right?
Margie: Yeah. And we are rebranding to Intentional Folk. The website will be intentionalfolk.com. But give us a week or two before that actually happens.
Tim Pickett: Intentionalfolk.com.
Margie: Our Instagram page if you want to see really good information with a lot of our products, a lot of our plants, you'll see more and more of the farm, is The Hemp Folk. It's just @thehempfolk, and again, that will be changing to @intentionalfolk. I think that this is so typical of this industry. I would love to be able to tell you that it's good. It's The Hemp Folk, and that's all I'm doing, but it can't. And it's not because I don't want to, it's just I needed to figure out a way to be able to sell products.
Tim Pickett: Yeah. It's always changing. That'll be the case for a little while, at least.
Chris Holifield: That's why you always have to stay on the news of what's going on in the industry, listen to all that podcasts, and news outlets, and so on and so forth.
Margie: So I would like to add one thing. Chris, can I?
Chris Holifield: Yeah. Of course.
Margie: I think that Tim definitely is more in the marijuana realm. And what I want to talk about is why I think ... And I'm not a medical doctor, but why I think CBD has a place for both smokable, ingestibles, and so forth. CBD, because it doesn't give you the head high, it does provide more and more of the pain relief. It helps with the inflammation, it helps with balancing out your endocrine system. So because of that I have a lot of friends who happen to also be more in the marijuana realm. And they're like, "Your products don't work." I'm like, "No. You just don't feel it, but the effects are there." That's one of the hurdles that I recently started to try to address.
Margie: I'm realizing that it's the older folks in the 50, 60, 70s that are starting to realize I want to not have pain every day, that are starting to take my products. And they're like, "This is the first time I've slept in three days ... for three days in a row for nine hours at a time in years." But they don't get the high. So it's hard to know if it's working. If you're looking for a high, you don't notice it as much. If you're looking to smoke hemp and then get high and to get an instant obvious effect, it's a lot harder to. You have to be ready for the small changes not for a big obvious one, like you get with THC.
Tim Pickett: You make a really good point and it's a good way to close out because you are right. And if somebody is looking for an introduction to cannabis, but they don't want to get stoned or high, then CBD products are the way to go. They're a good introduction, you can always try. You can always increase things, right?
Margie: Yeah.
Tim Pickett: You can always try things and then go to different products if one thing doesn't work, but it's a good way to try to introduce yourself to cannabis, it's CBD products.
Margie: In case people don't know, you can ingest cannabis, you could smoke cannabis, but you can also topically apply cannabis. It won't cure things, but holy crap. Is it helpful to reduce the pain?
Chris Holifield: Oh, yeah. After lifting some heavy weights or something like that.
Margie: Yeah.
Tim Pickett: It's restoring balance. The endocannabinoid system is a system for homeostasis, and sometimes you just have to supplement.
Margie: I'd much rather try something that's cannabis related, made from cannabis, versus something that's made from some new chemical that they came up with.
Chris Holifield: Exactly. I'm so glad we got you on the podcast, Margie.
Margie: Thanks, Chris. I'm so glad I could be here.
Tim Pickett: Thanks for coming on.
Chris Holifield: We'll have to bring you back through down the road and see how the farm is going-
Tim Pickett: Yeah. See how the farm is going.
Chris Holifield: ... and see how things are going.
Tim Pickett: Intentionalfolk.com. Yeah. This has been fun.
Chris Holifield: Your website, go check out your stuff, Tim. Utahmarijuana.org is how people can check out more of what you got going on, utahmarijuana.org/podcast is where people can listen to the podcast.
Tim Pickett: Yep. Utahmarijuana.org/podcast. All of them are up, Chris, and you release them every Friday morning 4:20.
Chris Holifield: Every Friday morning 4:20AM. Make sure you're subscribed in your favorite podcast player. If for some reason we're not in a podcast player, reach out to Tim or myself and let us know so we can make sure to get the podcast there.
Tim Pickett: Yep.
Chris Holifield: Otherwise, you have a good night, Margie.
Tim Pickett: All right. Stay safe out there.
I've been in the Utah cannabis space since the beginning of the program, in March 2020. In the early days of utahmarijuana.org, when we were finding our footing, I was primarily answering phones and scheduling appointments. (We had three employees and really no marketing department to speak of.) One phone call that stuck with me was a woman going through a very painful ovarian cyst. She asked, “Do I qualify?” I told her that she absolutely qualified — as pain lasting more than two weeks is a qualifying condition in Utah — and helped schedule her an appointment. She seemed insanely relieved to have another alternative to look forward to. Before she hung up, she said, “You know, being a woman at all should qualify you for Medical Cannabis, am I right?” I’ve thought about that about once a week since that day. Have you ever heard a truer statement? While cannabis is not gender-specific, there’s no denying its assistance and benefit when it comes to women’s health.
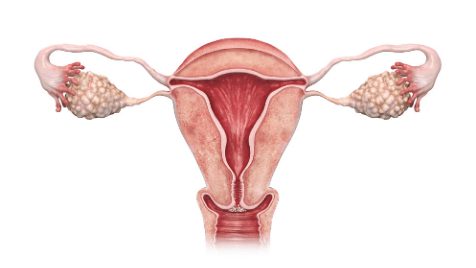 March is a big month for women. In addition to International Women’s Day (March 8th), we also acknowledge March 4th as HPV awareness day. Briefly, HPV, or the Human Papillomavirus, is the world’s most prevalent sexually transmitted disease — 80% of people will contract it at some point in their lives. It’s easy to spread because many go without symptoms and have no idea they have it. If untreated, a person carrying HPV runs a high risk of cervical cancer. In fact, HPV is responsible for 1 in 20 cancer cases all around the world. (Don't worry, though. There's a vaccine you can get to avoid it.)
March is a big month for women. In addition to International Women’s Day (March 8th), we also acknowledge March 4th as HPV awareness day. Briefly, HPV, or the Human Papillomavirus, is the world’s most prevalent sexually transmitted disease — 80% of people will contract it at some point in their lives. It’s easy to spread because many go without symptoms and have no idea they have it. If untreated, a person carrying HPV runs a high risk of cervical cancer. In fact, HPV is responsible for 1 in 20 cancer cases all around the world. (Don't worry, though. There's a vaccine you can get to avoid it.)
People have been self-medicating with cannabis for years and years. However, we have only just begun to scratch the surface with cannabis-related research as we make the shift into the medical world. In late 2016, it was announced that according to a study ran in Africa, cannabis may be effective in treating cervical cancer. They found that cannabis served as a preventative agent by reducing inflammation. This in turn is useful in reducing the likelihood of cancer. Similar to results found when testing RSO, or Rick Simpson oil, cannabis was found to inhibit tumor growth in vitro (a test tube or petri dish) and in vivo (a living organism). It should also be noted that inhalation of cannabis smoke does increase the risk of lung and colorectal cancer, due to the carcinogenic properties of combustion.
A far more common condition that women face monthly is the visit of Aunt Flo. While not all women menstruate monthly, it’s safe to assume that almost every person with a uterus has experienced unpleasant effects that accompany that time of the month. For a long time, much longer than we have research to support, women have been consuming cannabis to combat this unpleasantness. Fast forward to the 21st century and we can actually back that up with scientific evidence. Let me explain.
century and we can actually back that up with scientific evidence. Let me explain.
Whether you are a cannabis user or not, you have an endocannabinoid system. We all do. Simply put, your endocannabinoid system is a team of neurotransmitters and receptors that regulate everything from fertility to your ability to feel pain. The endocannabinoid system supports homeostasis in the body. Since this system is present in every human body (and some other mammals, too!), when cannabinoids like THC or CBD are introduced into your system, they naturally regulate your body’s responses to pain, mood, etc. Cannabis can also help relieve more severe pain related to endometriosis, etc. So, next time your red-headed cousin steps on the scene, see how she likes a cannabinoid cocktail. (In my own experience, a little bit of cannabis feels like it melts my cramps away completely. That’s the only way I can think to describe it, and I definitely recommend seeing for yourself. For longer-lasting relief, I like to take a gummy or two, depending on pain level. I always keep a vape cartridge near for sudden onset pain, too. At least for me, I never know how severe to expect my PMS symptoms to be, and I like to stay prepared.)
As of 2021, out of more than 39 million Americans who suffer from migraines, 28 million of them are women. In addition, a woman will experience a migraine differently than a man. Women often suffer for longer periods of time and suffer much more frequently. This is likely due to changes in estrogen levels and hormones caused by menstruation, some contraception methods, pregnancy, and menopause, though not all migraines are hormonal.
To give you a real-life example of cannabis use to relieve migraine pain, I’ll talk about myself again. I’ve suffered from migraines since I was 12 years old. Of course, I wasn’t self-medicating with cannabis back  then. By the time I hit high school, I was taking ibuprofen almost daily, or just suffering through it. (I’m also very anxious, and was afraid to overdo it and negatively affect my organs so early in life.) Around 16 or 17, as most people do, I began to experiment with cannabis for the first time. It was definitely for recreational purposes at that time, but I took a liking to it, and eventually found myself noticing the medicinal benefits during each session. Tension and stress often bring on my migraines, but I found that if I used cannabis when I started to feel anxious or stressed, those migraines would come far less often. However, if I medicated a bit too late and the pain had already arrived, sometimes vaping or smoking cannabis would make my headaches and migraines so much worse.
then. By the time I hit high school, I was taking ibuprofen almost daily, or just suffering through it. (I’m also very anxious, and was afraid to overdo it and negatively affect my organs so early in life.) Around 16 or 17, as most people do, I began to experiment with cannabis for the first time. It was definitely for recreational purposes at that time, but I took a liking to it, and eventually found myself noticing the medicinal benefits during each session. Tension and stress often bring on my migraines, but I found that if I used cannabis when I started to feel anxious or stressed, those migraines would come far less often. However, if I medicated a bit too late and the pain had already arrived, sometimes vaping or smoking cannabis would make my headaches and migraines so much worse.
Let’s jump ahead almost ten years and countless cannabis-related arguments with my mother, and I’m still a daily user. Now, though, I get to talk about it for a living and am using it completely legally. (Hallelujah! Thanks, Utah!) With a bit of guidance from my QMP, Tim Pickett, I learned new ways to treat my migraines. Tim introduced me to topicals, and my life changed forever. I’m not kidding. If I feel a migraine coming on, all I do now is rub a bit of my Cypress Sage Calm Balm from Zion Medicinal on the back of my neck, and within 20 minutes, my migraine has completely dissipated. 400/10; I cannot recommend topicals enough.
In conclusion, if you are a woman, you don’t have to suffer in silence any longer or poison your body with harsh prescription medications. There’s a natural alternative out there for you that I think you’ll find works as well, and in some cases, better than traditional Western medicine. You deserve a boost, a friend, a pick-me-up, a little something to get you through the day. Who run the world? Girls. And they’ve come prepared with THC.
In this episode of Utah in the Weeds, hosts Chris and Tim welcome Medical Cannabis patient and photographer Randyl Nielson. Their conversation with Nielson covered quite a bit of ground – ranging from mental illness to different strains and how cannabis helps Nielson be a better photographer.
Nielson suffers from a combination of PTSD and bipolar disorder. He explained how he can be depressed one day and amped up the next [05:51]. He also described the experience of feeling anxiety and depression simultaneously, and not having the right medications to deal with it.
The interview focused a lot on the mental health aspects of cannabis as medicine [15:07]. The hosts and their guest touched on the stigma attached to both Medical Cannabis use and mental illness. They also discussed how difficult it can be for doctors and patients to come up with the right combination of medications to treat conditions like PTSD and bipolar disorder. [32:54] For many patients, Medical Cannabis turns out to be the best option.
At the top of the podcast, Chris mentioned a number of podcast reviews they've received on iTunes. [01:53] Utah in the Weeds has been well received to date, which is something Tim and Chris are both enormously proud of.
The conversation with Nielson may very well be what you need to hear if you are thinking of applying for a Medical Cannabis Card but are worried about the stigma or what your family might think. Nielson speaks about that directly, referencing experiences he has had with his own family and neighbors. [38:34]
Episode 48 is an absolute must for mental health patients considering getting their Medical Cannabis Cards. If you are such a patient, take the time to listen. You will hear from someone who knows exactly what you're going through.
Chris: Should we start this off here, episode 48 of Utah in the Weeds. How are you doing Tim?
Tim: Yeah. I’m doing great, Chris. I'm excited to have people listen to this conversation. Randyl Nielson, who's a patient, and really got involved in the cannabis space in a unique way with his photography.
Chris: Oh man, his photography is amazing. Go check it out. We talk about that in this episode. We'll let you listen and get all of his links stuff but.
Tim: We'll give you the website at the very end.
Chris: Yeah. But you're going to enjoy this conversation. I was really excited to talk with him, especially about mental health, PTSD and how he's using cannabis for that. But before we get into that, Tim, I want to apologize that we never got a release for our live episode that we did. Was it last week that we did that, Tim? I guess it was last week.
Tim: Yeah, it was last on Friday, we did a Facebook live. And if you want to listen to that or you want to watch it, I think Facebook is the only place to get that at this point in time. Oh, and YouTube, you'd be able to go to Discover Marijuana on our feed on YouTube and rewatch that if you wanted to listen to that conversation. We had David Sutherland, a patient, JD Lauritzen was on, Cole Fullmer from Salt Baked City.
Chris: And he had a strain tester. What was his strain tester's name?
Tim: Oh yes. Yes, from Salt Baked City.
Chris: Wasn't that what he-
Tim: The funnest job on the planet, right? Just go test products and strains, Larson. Isn't the same Larson?
Chris: That sounds right.
Tim: Yeah. That was a fun conversation. Too bad it couldn't be released, but you know what? It is what it is. It's our first Facebook live and we'll do more. We'll dial it in.
Chris: We have some iTunes reviews that I wanted to read. We've got a couple iTunes reviews — I actually peeked this morning. And I was like oh my goodness, we got some iTunes reviews. So I want to read those really quick if that's okay, Tim.
Tim: Absolutely.
Chris: The first one was left by Weightlifter Z and they say “Absolutely amazing.” They say “my wife has been using medical marijuana since it became legal here in Utah. I recently started using it as well for ASD and my life has changed. Please keep making these, if you can sometime do a show talking about the strange you can get at the pharmacies that have and what they are good for I would love that. Also happy to come on the show, if you ever need a guest.” Hey, so that's actually a good idea. We should do an episode about a lot of the common strains.
Tim: Yeah, absolutely. We should gather up all the strains that we've tried and that are available and we should just go through them.
Chris: Yeah, no, that was a good recommendation. The next one was left by Aaron 5634. And she says, “I'm not in Utah, but love this podcast.” And she says “as a cancer patient who uses medical cannabis, I learned so much from this podcast. Thanks guys. Keep up the good work.” Hey, so that's awesome. They don't even live in Utah and they listen.
Tim: That's sweet. I'm glad that people are getting something out of this. I think our patient's stories are good. It's nice to go someplace and listen to people's stories that might be like yours. This one today with Randyl, if you have PTSD or you have bipolar and you're on this journey to learn about cannabis and what works or what doesn't for people, this is a good conversation to start with.
Chris: Utahmarijuana.org/podcast is where people can listen to podcasts. Right?
Tim: Yes. And they can listen and read all 48 episodes. They are all there. We are all caught up Chris and yeah, again, and if you want to connect with me, Utahmarijuana.org, you can chat with us and go listen to Chris's other podcast I am Salt Lake.
Chris: Yeah. Iamsaltlake.com. Go check it out. We've been chatting with some really fun people on that one as well. A lot of local food artists in food restaurant tiers, chefs, people like that. So go give it a listen.
Tim: Absolutely. And then you can come see us. The last thing I'll say is you can come see us at our new Bountiful location, Utah Therapeutic Health Center Clinic, right next to Wholesome Co Cannabis company in Bountiful in the same building. So you can get your renewal or get the evaluation and introduce you right to the product right there in the same building. Super cool.
Chris: Yeah. Just drive to Wholesome, you'll see a sign. I saw a sign there the other day when I went up there.
Tim: Yeah. A sign right upfront. You can come see us.
Chris: It's cool. Let's get into that conversation with Randyl, Tim. And thank you so much for listening to everybody. Enjoy the conversation.
-----
Tim: Tell us a little bit about you, who's Randyl Nielson?
Randyl Nielson: Well, that depends on how much time you want to spend. I'm from a small town in central Utah called Oak City. I grew up there till I was 18, it's 600 people. So pretty small close minded town. Went to high school at Delta High down there. Did a lot of things that I regret obviously as most adults do looking back at high school but-
Chris: Maybe.
Randyl Nielson: ... It was an interesting place to grow up. I was a bit of a counter-culture person there. I wasn't really well liked by a lot of people. I was a skater punk kind of kid. So I was kind of on the outside scene of things. I got into drugs and stuff when I was younger, kind of broke out of that as I got older, got married, divorced, married, again, I've been married now for 18 years to an amazing woman who's dealt with more than I could possibly imagine anybody could deal with.
Randyl Nielson: But so I got remarried. Right after was when my mental illness kind of kicked in. Our first son passed away after a couple of days and it didn't affect me right away. It took three or four years before it really kicked in, but when it kicked in, it kind of broke me. I was in the middle of school trying to get a degree and somehow I managed to get through it. I didn't get diagnosed with PTSD and bipolar until my last actual semester at school. And so I was dealing with a lot of crazy stuff during that time. And right before that had happened, I had injured myself and got on some opiates, got pretty heavily hooked on them after being clean for eight years and overdosed one night. And I hadn't told my wife anything about what I was doing.
Randyl Nielson: And so it was a surprise to her. She didn't really know what was going on. And it was a real wake up call to me that I had gotten in over my head more than I really thought that I was going to. As a drug addict, you kind of underestimate your involvement in things, I guess. So the next day, literally the next day, a friend of mine got me some cannabis and it was the first time I'd used cannabis in eight or nine years, but it kind of started me on the path of dealing with things a little bit better. It got me off the opiates right away. After that experience, opiates now kind of make me sick which is absolutely wonderful.
Randyl Nielson: I don't know if it's kosher to say, but I've been getting cannabis from the alternative market ever since to treat pain, as well as the mental illnesses that I'm dealing with. For work, I guess you want to know about that. I'm a photographer/designer for climbing hold company. It's a pretty awesome job. I get to do a lot of really fun stuff. And the photography work I do there kind of blends into the cannabis work and I learned stuff from both aspects. And so it's a really fun way to kind of make the two work together, I guess.
Tim: We'll get into this a little bit later in the interview, but people are going to want to know your photography is currently on display at one of the local pharmacies. Right?
Randyl Nielson: Yeah. I was up there two weeks ago and I saw it in a display case at Beehive up in West Valley.
Chris: It's beautiful.
Randyl Nielson: Thank you.
Chris: It is some of the most beautiful photography. Your Instagram photography is beautiful too, but the stuff at Beehive is beautiful too.
Randyl Nielson: Thank you. It's been a really fun thing to explore. I've been shooting for 18 years and it's a whole new world of photography that I've had to learn.
Tim: Yeah. That close up. Okay. So describe that a little bit. We got to talk about this a little bit. We're going to have to go back to the mental health.
Randyl Nielson: Okay. That's fine. That's fine. What do you want me to describe exactly?
Tim: I mean, how do you capture such close up shots, man? You could see every fiber of the cannabis leaves.
Randyl Nielson: Well, I bought a really, really nice lens. It's a one to five X macro. And so 1X macro means that's what your eye sees one-to-one, right. And a 5X is five times that size. And so the pictures you're seeing with the trichomes kind of standing out in the light and stuff like that. It's usually at 5X or I've put a doubler on it. And so it's very close.
Randyl Nielson: I'm working maybe a centimeter away from the plant, right. And some of those pieces that I'm working with are no more than a quarter inch big. So I've got it jabbed on a little pin sitting there on my table. And then the way that you get the actual detail is a technique that I just learned this last fall. It's a focus stacking technique where you take a picture at the front of the image and then you take pictures throughout the image until you get to the back and your focal point moves as you go through that. And then in software afterwards, you stack those together and it makes it so the entire thing is in focus.
Tim: Oh, this kind of makes sense. Now, I'm going to really take a leap here, Chris. Do you feel like the work that you're doing with the cannabis — you're getting so close to this — it really just seems this would be a cathartic project?
Randyl Nielson: Oh yeah.
Tim: I used to have a woodshop and you could go in there, you put the headphones on and you could build stuff and you're just in there. Right. Do you feel that is your photography is that kind of therapy for you?
Randyl Nielson: 100%. Up until, I mean, I always shoot landscapes and wildlife and stuff like that. I'm a big bird nerd. I take pictures of birds all the time, but I've really struggled since I got on medication for my bipolar anti-psychotic. It kind of killed that creative drive that I had flourishing during school where I'm surrounded by artists and creating all the time. So it's been years since I've really gotten involved in a project photographically that I kept going back to again and again and again. And yeah, this cannabis thing I started last, I think it was spring once I first got my first legal purchase in Utah. It was April, I think I used my recommendation letter to go up to Dragonfly. I started shooting it then and it was a way to kind of connect and show other people the quality that we're getting here because there's a lot of negative talk out there about how ghetto the quality of flower and stuff is here. And I mean, I've been to States where it's legal and yeah, there's stuff that's super high end but we're getting there.
Randyl Nielson: And so I kind of want to show that off, the naysayers that are like yeah, this bud is no good. And it's well, I don't know. It looks pretty good to me, but it's been super cathartic to just... I have this crappy little office here, but right behind me I've got a table with a studio set up, I've got lights sitting here, I've got a blackout curtain, I've got multiple backdrops. So I can do everything just sitting here in my office and the kids can be doing their homework, my wife's painting or drawing or whatever. And I can just shut the door and spend four or five hours through the process of taking all those pictures, stacking them, finding the right flower structured, oppose the calyxes, the stigmas stuff like that. Searching for little track homes, standing out that I can find and it's also kind of fun to vaporize that flower while I'm actually shooting it and get kind of a little bit more of a connection with it. Understand it a little bit deeper, I guess kind of sounds hippy-ish but-
Chris: Yeah, man. You got to become one with it.
Randyl Nielson: Yeah. I mean, you have to do that with any subject that you're really trying to understand photographically. I mean, if you're shooting photos of a person, you have to talk to them and get to know them a little bit and understand them in order to really capture the essence of who they are in a photograph. And I've kind of approached this flower project as the same way as a portrait's set up where I'm actually setting up the lights very similar to a portrait setup and I'm posing the flower if you will, trying to define these really weird little shaped clusters of calyxes and stuff like that, that are kind of an abstract, but also really cool looking because they're covered in trichomes and hairs and all sorts of stuff. But yeah, it's something I have a hard time not doing it.
Tim: Yeah. It draws you in to the point where like I said, at the beginning of our discussion here we'll get to the photography, but it just draws you in as it's such a cool thing. I've got one as my screen saver.
Randyl Nielson: That's amazing to hear. I love having people connect with my work, whatever it may be, but I've gotten compliments and stuff like that through my Instagram page, but the coolest thing that's come from it is I've shared a little bit of my bipolar and PTSD on there in posts, but I have people coming to me, messaging me in the private messages that are asking me for suggestions on flower, on what works for whatever symptoms they're trying to treat. Asking me for advice on different things. And it's probably the coolest thing that's come out of this is being able to connect with other people and just say, yeah, this works for me because of this and this.
Randyl Nielson: I try to treat the flower strictly as a medicine when I'm using it. I try to analyze the effects that it's having on me and the symptoms I'm treating with it so that I can say to someone, yeah, this is what I was doing and not sound like a fool.
Tim: You mentioned before that you were on some antidepressants and some anti-psychotics and one of the kind of depressing side effects of those medications is this downregulation of creativity, kind of this —really it just kind of makes the world gray. It takes that's how I've heard it described. And do you feel with cannabis that has brought back that, that's how you've gained this creativity back?
Randyl Nielson: It's been essential in my work as a wall designer. I don't know if people understand what I'm saying, indoor climbing gyms. I designed the grips that go on the wall. So I shaped them out of foam. And then I worked for the company that we mold them and put them out and sell them whatever. And so I spent a lot of time in my garage, basically sculpting foam. And when you're on the down swing of a bipolar episode, and you're just so depressed, you don't care about much, but you still have to be creative. There's no way I could do it without cannabis. It takes away that flat feeling from the depression. And it allows me to be in the moment more rather than being stuck in this fog.
Tim: I've been doing a lot of research on mental health and cannabis and aware in the brain it works and this. I mean, you're upregulating things and you're downregulating things. But one of the things that we are trying to counteract is these effects of the typical prescription medications, because those they're just harsh side effects. They tend to work in some ways and for a lot of people, but the side effects are just so harsh. And so trying to find a balance in mental health treatment with cannabis is a very up and coming field with really interesting brain research. Have you decreased your medications or changed them because of the cannabis?
Randyl Nielson: I've definitely. So I had a prescription for Xanax for anxiety, panic attack type stuff. I used it three or four years ago we went out to New York, New Jersey for a vacation, and I didn't have any cannabis with me while I was there. And so as I was dealing with extreme anxiety, I was taking that and it was making me feel better in one way but worse in other ways. Luckily by the end of the trip a very kind friend out there had found me some edibles from someone who was a medical patient in New Jersey. And I was able to actually relax enough to enjoy the flight home and not be miserable the whole time. I'm very happy to be off of benzos. I hate them. I try not to use them anyway, but ever since I've been buying medically in Utah I have not had to take a single Xanax.
Tim: There you go.
Randyl Nielson: As far as the atypical anti-psychotics and stuff like that I got really lucky that I only had to go through three or four meds before I found one that worked. And then just recently we added an antidepressant so that I could kind of stay out of those nine months long, mild depressions that I tend to get into. But the cannabis is a very, very active part of my treatment plan.
Randyl Nielson: I have a variety of not only different types of flower, but I have tinctures and edibles and vape pens and stuff like that, so that I can tailor exactly what I need for the symptoms that I'm dealing with. Because with the PTSD/bipolar combo, sometimes you just don't know what the hell you're going to find when you wake up. You can be happy and having a good day and you wake up the next day and it's going to be three or four weeks of pure hell of being miserable and depressed, or even worse getting into a mixed episode where your anxiety is amped up. And the cannabis is essential in calming me down.
Randyl Nielson: The way that I used to describe it to my wife before she got her med card and got to understand how it works is it's like a nerve blanket. So it's my nerves are just fried, they're frazzled, they're raw. And it's like somebody just put a blanket around those nerves and just calmed them down and helped me relax.
Chris: It's a good way to explain it.
Tim: That is a good way to explain it. Have you been able to get the product that you need around town all the way since — we see Dragonfly have in their year anniversary all over social media, right? We've been doing this a year.
Randyl Nielson: During the pandemic — I'm sure you guys experienced it or understood it — the whole show-up-at-Dragonfly-and-wait-for-four hours. Because I drove up from Utah County, I wait in the car for four hours because I've got no other option. And then I'd spend 500 to 1000 dollars because I don't want to come back up for a couple months.
Randyl Nielson: And so once the other pharmacies started opening up, it was hard for me to get out of that mindset of having to stock up. I literally drive by Deseret Wellness on my way to and from work every day, it's one of the biggest blessings in my life. I can just stop on my way home and say, I need some tincture today, I'm out. And they've had pretty much everything that I've needed most of the time. I mean, there's obviously been some shortages of flour here and there and it's been a little bit slow going, getting the RSO and the concentrates and things like that going, but other than maybe needing a little bit more on the concentrate side of things I've been pretty happy with everything that I've been able to get ahold of.
Tim: Do you like those guys down there at Deseret?
Randyl Nielson: Oh yeah. They're great. They're awesome. Yeah. I love going there. I dropped off a few photos to them just so that they could put them in their break room and stuff. And so we always talk about that kind of stuff when I go in, it's great.
Tim: I know, right. At Beehive, your backgrounds are all black and the vibe in there is a little different down at Deseret, the vibe is white, you don't have to have a white background with your-
Randyl Nielson: I can do that. Yeah. It's definitely doable. But yeah, I like the way things are starting to pan out. It would be nice once the other pharmacies down South open up, so that there's a little bit more option if I'm traveling that way. But if you're prepared it's not that big of a deal anyway, because I don't have to worry about driving with cannabis anymore.
Chris: Isn't that nice?
Tim: Yeah. Isn't that nice?
Randyl Nielson: Yeah. I don't medicate before I drive, but if I'm going on a three hour drive, I know that by the end of it, I'm going to get there and I'm going to get medicated and I'm going to feel better. And so it makes that drive a little bit more tolerable.
Chris: What's your favorite way to consume cannabis? You mentioned all the ways. Okay, so vaping. Okay.
Randyl Nielson: Yeah. Dry herb vape is my favorite. I love the whole plant aspect of it.
Chris: What Kind of vaporizer do you have right there? What was that?
Randyl Nielson: This is Arizer Solo 2.
Chris: I'm not familiar with.
Randyl Nielson: A-R-I-Z-E-R.
Tim: A-R-I-Z-E-R, Arizer 2. And it looks like it got a pretty good sized battery there.
Randyl Nielson: So this one it's not awesome for being portable as far as outside the home, but for being in the house and walking around, it's amazing. It's about a three hour battery life, but you can also use it while you're charging. My favorite thing about it is it's an all glass vapor path. So the flower never touches anything besides glass. There's glass stems that you pack flower in the end and then you put it down in the chamber and it's got a convection air coming through and heating it up as you draw.
Tim: People who get into vaporizers, they end up in this glass or ceramic thing. Don't they? Right. The taste is-
Randyl Nielson: It's all about, I mean, the flavor is amazing.
Tim: The flavor is a little bit better. The draw with your vaporizer does the draw have to be really slow? The Firefly is, it doesn't have a glass all the way through, but the draw has to be so slow to get that air to warm the plant.
Randyl Nielson: No. It's got this jet fire thing at the bottom of it. And so the chamber is heated partially, but then it's got the heat jets underneath so that as you draw it just heats it immediately. So the only thing that affects the draw is how tightly you pack it.
Tim: Did you get the vaporizer here locally or did you have to order it?
Randyl Nielson: No, I ordered it. This is actually I've had three of theirs so far. I have a smaller portable one that I gave away to a friend and I just ordered another one two weeks ago and they still haven't gotten it to me. So if you're going to go for Arizer, do it from Planet of the Vapes or another second party, their customer service isn't great. Their products are amazing.
Randyl Nielson: But yeah, as soon as the law was passed, two little over two years ago, right? It was December that it happened. I got a letter of recommendation from my APRN, my psych APRN. I've been working with her for seven years now. We're very well versed on what works for me and what doesn't. And so she's very supportive of this. She's actually become a QMP recently. So I'm going to have her taking over my card recertification stuff. But yeah, as soon as that law passed, I bought a vaporizer and I stopped smoking. And I tried it once since then and it tasted I was sucking on an exhaust of a car.
Tim: Yeah. I think I wish everybody had that experience, huh Chris?
Chris: With what? Smoking it.
Tim: With smoking it. Right. There has been some-
Chris: I don't know if I'd say smoking on the exhaust of a car though, that's-
Tim: Well, yeah, for sure.
Randyl Nielson: I'm talking like the flavor was just not there from the smoke and my lungs hurt the next day. My mouth tasted I had drank hot coffee and burned all my taste buds off. It was such an unpleasant experience that I'm just like, yeah, I'm never going to do that again.
Tim: We're going to put you on a commercial for the department of health. I'm calling-
Chris: They love you all of a sudden.
Tim: They love you.
Chris: No, I mean you speak a lot of truth because I used to be a cigarette smoker and now when I get around cigarettes, I'm just like, oh, that's disgusting. What's going on?
Randyl Nielson: I was the same.
Chris: When you're part of it, you don't think it's going on until you pull up.
Tim: Do you guys still get that craving though of cigarette smoke? You walk around somewhere and you'll smell somebody smoking cigarettes. And you're like, "Oh man, that just smells it would taste good."
Chris: No, not really.
Tim: Am I the only one that happens to? Dang.
Randyl Nielson: On a very rare occasion.
Tim: Should I have not admitted that?
Chris: No, I hear people that that happens too, but it just doesn't happen to me luckily, so.
Tim: I don't know. I think it's because I grew up with some smokers and so it's got some sort of limbic system, some sort of emotional brain connection for me. Right. It brings me back to some childhood thing where I was like, oh yeah, my family smokes.
Chris: So did we ask what your favorite strain is Randyl, what's your favorite strain, your all time favorite strain that you're enjoying, or at least strain you're enjoying these days?
Randyl Nielson: All-time favorite it's kind of a tie between Afgoo and Durban Poison, because Afgoo I haven't been able to find it in years, but it's just mind-blowingly good. It's amazing.
Randyl Nielson: But the Durban Poison that came out from Standard Wellness last fall, I stocked up on that when it came out because it was fire. I actually just vaped the last of mine a couple of days ago. It's been fantastic. But as far as being able to regularly go back and get medicine, Dragonfly Lava Cake, and now I recently got the second round or maybe the third round of the Standard Wellness Miracle Alien Cookies. And they both have the same effect on me as far as anti-anxiety and being able to just kind of calm my overactive brain.
Tim: Is that the same with Durban Poison? Because isn't Durban Poison a pretty good sativa?
Randyl Nielson: It is, but because it's a land race, it acts very different than almost every other sativa. I picked up some of the Good Sun Green Wildfire, Green Crack. Yeah. That stuff gives me some anxiety and I have to use it when I'm depressed and I need that upper. It's great for that. But the Durban Poison, it calmed me down. I don't know why, it was great.
Tim: This finding that equilibrium man, finding the equilibrium, finding that happy place with the flower and all that's going on in there, the entourage effect. Yeah. That's cool that you're using different strains for different types of things. And I think it's good for people to hear too, right? That Green Crack. I mean, yeah it can give you a little anxiety so you got to watch out.
Randyl Nielson: Yeah. Definitely.
Tim: For some people Durban Poison would be the same way, right?
Randyl Nielson: Yeah. I talked to, I think one of the pharmacy agent over at Deseret. And he said, yeah, it gave him a little bit too much anxiety. He didn't really like it that much, but my wife who has high anxiety as well it was the same thing for her just completely calm and relaxing and yeah.
Tim: So interesting. Just goes to show you that it's so self... You have to give yourself permission first of all, to experiment with your medicine. And this is so foreign to people.
Randyl Nielson: Well, it's bizarre. Yeah.
Tim: But on the other hand you said it in the beginning of our interview, you were lucky with bipolar and it took you about three medications to find the right one. So most people with a bipolar condition or a severe mental health condition they might try three, four, five, six different medications over the course of a couple of years, right? Mind you, a couple of years in order to find the right medications. And so is it that much different that we're trying different strains, different delivery methods, different consumption method? With cannabis I can see there's an argument that it's not that much different, except you have to give yourself permission to experiment.
Randyl Nielson: It's the stigma, right? We're not supposed to be doing this anyway because it's federally illegal. And so for me, most of my life, it's been something that you don't talk about. There's the code, you can tell that guy's a stoner but you don't really talk about this kind of stuff because you don't want to be prosecuted for it. Right. You don't want to get in trouble. And so yeah, now you have the ability to say, hey, I can go do this. I can go to the store. I can try this out. If it doesn't work for me, I can go back and try something else and I can drive too, and from there comfortably, knowing that if a cop pulls me over, he's gotten-
Tim: Isn't that awesome?
Randyl Nielson: As long as I'm not medicated, it's a miss.
Chris: Have you run into any problems with the law since anything or, I mean am just curious.
Randyl Nielson: I have not. I kind of anxiously awaiting excited, but not. It's just nice to have that. I had a run in with law enforcement. It was right before I got diagnosed. I was self-medicating and I was being dumb on a manic tear. And I ran into law enforcement and got charged.
Tim: Charged with cannabis with possession.
Randyl Nielson: Not have that anxiety — Yeah. I got charged with possession and paraphernalia and to not have that paranoia and anxiety of are my neighbors going to smell it I'm out in the garage. Are they going to know, are they going to call the cops? It's hard to really let yourself have permission to medicate when nobody else wants to give you that permission. And so now that we have this law that says, yeah, go do it, go try to find something that works for you. The only thing that's weird about it is it's kind of you go figure it out. Maybe you talk to your pharmacist or you talk to your doctor a little bit, but it's still kind of just an experimental thing. Whereas with pharmaceuticals, they've got a longer history of what it can treat. And so they can put you in a little bit better general direction right away, theoretically.
Tim: Yeah. Theoretically you kind of have this is the algorithm and this is how you treat it. This is beside you don't have EVS system to work for you.
Randyl Nielson: Right.
Tim: You can just write a prescription on my side and you just write a prescription, they can take it down. They can fill it and they can start feeling better.
Randyl Nielson: Well, I mean, a perfect example is for bipolar, the go-to is lithium. Right. And it has been for years, there's some horrible side effects from lithium and you have to monitor it all the time. Right. And so it's like we're saying they have that general direction, but they're still kind of spitballing and like well, let's throw this at the wall and see if it sticks. No, that one made you sleep for 16 hours a day, that one's not going to work. Let's throw this one. Oh, that one made you feel like you wanted to tear your skin off. Maybe that one's not a good one. The advantage of doing it with cannabis is you don't have those negative side effects.
Chris: This one give you the munchies and this one.
Randyl Nielson: Right.
Tim: Yeah. Oh, this one made me take a nap. This one made me watch Ferris Bueller. This one gave me anxiety so I'll stay away from that one. And this one made me shoot these amazing photos, let's stick with that.
Chris: The worst thing anxiety there. You just listed a bunch of stuff that happens but like the-
Tim: Right. I mentioned-
Chris: Tearing my skin off.
Tim: ... Yeah. But the worst of that is like... That's like, oh, I used the wrong flower and I have three hours of anxiety. I don't have two days or two months of anxiety trying to get used to this medication. That's the other thing about traditional medications is the standard education is, okay, start with this dose will ramp up to this dose. If you feel bad, side effects, we'll cut you back. We won't stop it and change it. We're just going to keep you on it. This is a three month trial. This isn't a three-day trial. We're going to give you this for three months, measure your liver function. Right. So you don't get lithium toxicity. You don't end up in the hospital.
Randyl Nielson: Yeah. It's scary shit man. You read those warning labels on some of that medicine and you're like, I really don't want to take this, but-
Chris: What are my other choices? Well now your choice is medical cannabis.
Randyl Nielson: Right. So benzos, perfect example. They're one of the worst things to come off of once you become dependent on them. There are people that have literally killed themselves because they were under so much extreme pain in one way or another coming off of those drugs and to not even have to deal with that is a huge blessing. To be able to say I was telling Chris earlier, before we started recording yesterday was actually not a good day for me to do this. So today works out better because yesterday I was super high anxiety. I had to take a high dose of that standard RSO. And it didn't even kick in until fully until our interview would have been over. But I know that it works for me. It's not as instant necessarily as a benzo, but as far as treating my anxiety symptoms, a high dose of edibles does the exact same thing only better.
Tim: How often do you have those days with your conditions and do you think that those days are decreasing overall?
Randyl Nielson: It depends. It's kind of situational. My PTSD is fairly complex. There's death and then I rolled a car a couple of years ago. And so driving is an issue for me and there's a lot of issues that go into my anxieties. And whenever I'm in an elevated or lowered mood state from the bipolar, it ramps up those anxieties quite significantly. And so it's something that I still deal with fairly regularly. Maybe not every day, maybe not every week, but it definitely happens pretty often. I worry about my kids walking home from school still, pretty heavily to where I check the ring sometimes in the middle of the day to make sure they made it home, just because I have that anxiety about a child dying, therapy has helped immensely.
Randyl Nielson: It's helped me be able to actually talk about it without breaking down. But I don't know, I was up skiing with a friend the other day and he asked me, he's a doctor, an ER doctor. And he was, "Do you think you're ever going to get past this?" And I couldn't give him an answer because I don't know. I know that I'm at a point where I can function with it and get through life and not have it break me apart like it used to, but it still affects me fairly regularly.
Tim: This idea of getting past it might not be the right way to, in my opinion, this is my opinion about behavioral health, but might not be the right way to look at it. Your over time if you can try to tell yourself a new story, right? That's what we're trying to do with behavioral health. And with these mental health therapies is trying to allow the patient to not have to avoid certain situations like you. If you roll the car, we've got to have you be able to drive a car and avoid driving a car. So we need to learn that behavior, but we need to learn a story. We need to teach the brain a new story. The new story being your kids are coming home, they're safe. You're going to get to the store in your car, you're safe. Right. And that seems to be time-related plus all of these therapies.
Randyl Nielson: Yeah, definitely.
Tim: But I'm not sure we want to understand it, get past it.
Randyl Nielson: Get past it to me, there was a study that I read recently about how they're starting to understand how cannabis helps with PTSD and it helps rewrite those traumatic memories, like you're talking about to rewrite that story. And to me getting past it is getting past those triggers. I was triggered the other day by just a random situation being in the wrong place at the wrong time. And something just snapped in me and I had to leave and go kind of collect myself. And that's what I mean by getting past, I want to get past the point where I have to worry about that as much? And like I said, that depends a lot on therapy, but also on medication.
Tim: Oh, totally. And cannabis makes it easier to not have to avoid those situations. Right?
Randyl Nielson: Right.
Chris: You were mentioning not having to hide smell of cannabis with the neighbors and friends and dah, dah, dah. I mean, are your family and friends and whatnot pretty supportive of your cannabis use? Or are you still kind of, don't talk about it or what's that situation. You were mentioning your wife is a medical cannabis patient as well.
Randyl Nielson: I'm not shy about it. I don't openly go to my neighbors... Actually I guess I did. My next door neighbor.
Randyl Nielson: After I got my card and I just said, "Hey, man, just so you know if you smell anything, it's legal, don't worry about it you don't need to call the cops." He's like, "Cool, no problem." I have other neighbors that wouldn't react the same way. So I haven't approached them about it. I'm more than happy to discuss it with them if they feel it needs to be discussed. My family's very supportive. My mom now that she understands kind of more about it, she's very supportive of it and very glad that I'm doing it. My dad is actually looking into maybe getting a medical card for himself. He's got metal plates in his back and different things like that. And so he's actually starting to look into it, which is a surprise because I didn't think that that would ever really happen. But yeah, I'm pretty supported in it and I'm pretty glad.
Chris: I was just curious because I know a lot of people, a handful of people that I've talked to they're interested in it, but they're nervous of what their family might think and they don't feel they have anybody to talk to about it. I don't know and I'm sure Tim's seen similar people like that or talked to people like that.
Tim: Oh, yeah.
Chris: I'm sure it's common here in Utah. I live in Utah. I mean, no offense. It's like this is Utah and people don't know how to use cannabis or how to even approach it.
Randyl Nielson: How to even approach it. Yeah. And that's why for me I'm not judging anybody for smoking or doing anything. That's not spot on with the law. For me I try to follow the law as well as I can to the letter so that I'm promoting it as a medicine and not as somebody just getting high because that's the big argument from everybody against it was, it's just going to turn into recreational. And in my eyes, if you're posting on Instagram, you're doing bong loads with the lighter that's smoking it and you signed a document that said you weren't going to do that.
Randyl Nielson: And so I think being on point with it and following those rules and treating it like a medicine that's what kind of brought my mom around and made her more understanding about it with saying, okay, mom, here's the law. This is what I can do. This is what is allowed. And the fact that I wasn't smoking it around her and stuff like that, I think it really had an impact and helped her understand a little bit better that people in Utah are trying to treat this as medicine, not just as a subversive way to get recreational weed.
Tim: Again, can we call the department of health —
Chris: Give this guy a job.
Tim: .... And have you be their spokesperson. I just want to-
Randyl Nielson: If they want to pay me, let's go for it.
Tim: I don't disagree with you at all. I think that you have hit the nail on the head when it comes to de-stigmatizing the plant for Utahs. It's about laying out the rules, laying out the benefits, the risks, saying that it's legal, educating people about it, and given them access.
Tim: And then treating it like another tool in the toolbox from my side, the provider side. Right. And then see what happens.
Randyl Nielson: Yeah. And I think even a big part of that is just how we talk about it. What words we use to describe it, right. If we're saying, "Hey, I got to go get my weed." Somebody is going to be like, uh. But if you're like, "I've got to go pick up some cannabis, I'm having some anxiety." They tend to have a little bit more understanding and like, "Oh, okay. Yeah, that makes sense that it would be something that you could do."
Chris: Yes. What would you tell somebody who's listening that might be a little apprehensive about trying it? What would you tell them? They might be a little skeptical.
Randyl Nielson: My wife was even after I got my card or had my letter and got my card, she was still a little bit skeptical about using it for herself about getting her card. And I'm like, "Hey, you've experienced the same trauma that I have. It's okay for you to go and find something that helps you treat this anxiety that you're dealing with on a daily basis." And for her it was taking away that whole smoking aspect and turning it into a medicine. We're going to go get you some gummies. We're going to start you at 0.25 milligrams so that you don't freak out. Because even that five milligram can make some people really turned off to cannabis as medicine. They're like, no, that was too much. I can't do it. But you go two and a half it's nice to see some of the smaller doses coming for those kinds of patients.
Randyl Nielson: Some of the tinctures, my wife has one of the Boojum sprays that's only 2.3 or 2.4 milligrams per spray. And so for her five milligrams is her max. She doesn't want to take more than that because it makes her feel loopy and out of control. And that five milligrams is almost too much to be able to go do the things she needs to do throughout the house and throughout the day. And so if she takes that two and a half, she knows that her anxiety is going to be lessened, but she's not going to have that messed up head that she's trying to avoid.
Tim: Yeah. Thanks to Boojum for those sprays.
Randyl Nielson: Their tinctures are amazing.
Tim: We're going to review those and their tinctures are pretty good too.
Randyl Nielson: Everything about their tinctures and sprays are amazing. I have one in office at all times.
Chris: Did you catch that episode we recorded with... What's his name, my mind? Dashiel, yeah.
Tim: Dashiel.
Randyl Nielson: I haven't had a chance to listen to that one yet.
Tim: Yeah. It's pretty good. You got to listen to that one, we talked to them about the Boojum tree and their whole outlook on things and they've got some legit products. I read their research papers and yeah I really liked that company. I like their products.
Randyl Nielson: One of the great things about them besides their products is in their social media, they're doing everything they can to educate patients about why they're putting what they're putting into their product and why it should be helpful for you instead of just here's a tincture, it's got some THC and CBD good luck. They're saying here's a tincture with citral in it. The citral does this. This is why you want this one. If that doesn't work, go get the merci in one or the limonene in one or they're starting to tailor it for exactly what people need.
Tim: It's pretty cool idea. And their products are really cool.
Randyl Nielson: Yeah.
Tim: So Randyl, what's your website. Do you have a website up for people to connect with you or to see your photography?
Randyl Nielson: Yeah. It's nielsonphoto.com, N-I-E-L-S-O-Nphoto.com. Just my last name. And right now I still have to go figure some things out. I got it roughly thrown together the other night because I was worried you'd asked me about it.
Tim: Yeah.
Randyl Nielson: I just updated all the photos. I had a bunch of old stuff on there that wasn't that cool. And so I updated it recently and got some of the more recent macro stuff on there.
Tim: I'll tell you what if you have listened all the way to the end of this podcast, then you have got a treat because nielsonphoto.com, I am on it right now. And I'm telling you what these photos are fire.
Randyl Nielson: Thank you.
Tim: They off the hook. I mean, trichomes in detail. You've got that brown. I don't even know what to call that. That tail off the top of the flower.
Randyl Nielson: I think that's the stigma.
Tim: The stigma. I mean, these things.
Randyl Nielson: A little hair thing out.
Tim: They're so awesome.
Randyl Nielson: Thank you.
Tim: Yeah. People are going to love this.
Randyl Nielson: I don't want to get any hopes up, but I did just receive from China today an adapter for a microscope objective for my camera so that I can get way beyond that 5X magnification and get in there even further.
Tim: Oh yeah.
Randyl Nielson: So it's becoming a little bit of an addiction. I'm spending-
Tim: You're buying microscopic lenses from China, then yes.
Randyl Nielson: That's the only place I could find what I needed sadly now but —
Chris: You need some of these photos in your office, Tim.
Randyl Nielson: Yeah, it's-
Tim: Done. This is on the list. There's no question that you're going to be able to see these photos in my office.
Randyl Nielson: I'm not 100% sure if it works yet, I'm trying to set it up so that people can buy prints off the website. I don't know if anybody's going to have a problem printing pictures of cannabis. So I've got to make a test printer too and order and see what —
Chris: Dude if you took these somewhere they wouldn't even know what it was.
Randyl Nielson: If that works out.
Chris: Like if you just, yeah.
Randyl Nielson: Well, that's the thing. Yeah.
Tim: I agree.
Randyl Nielson: That's true. With the macro ones for sure.
Tim: Yep, for sure. And we're going to put a blog post together about this because this is so cool.
Randyl Nielson: Thank you. I love this plant, man.
Tim: This is really cool. I'm sorry. I'm getting sidetracked.
Chris: Tim's looking at weed porn.
Tim: I am mesmerized by this photos. Sorry, I'm looking at weed.
Randyl Nielson: I'm okay with that. I will not complain.
Tim: It kind of is, I mean, that's really what it kind of look-
Randyl Nielson: Yeah.
Tim: Sorry.
Chris: But cool man, go check out his photography. When I saw that you were interested in coming on the podcast, Randyl, I was like man, I already love his Instagram stuff. And so that was why I was just like —
Randyl Nielson: Thank you. I appreciate that.
Tim: Your outdoor photos are cool. Your story is great. I'm really excited for you. I think I'm just so happy that you found that creativity again through cannabis.
Randyl Nielson: Yeah.
Tim: That's just exciting.
Randyl Nielson: It's a game changer for sure. I wouldn't be able to do what I do for work without it. There's times when my mental health doesn't want me to do anything and I have to do it and cannabis usually almost always makes it happen.
Chris: Anything else you want to talk to him about Tim or anything you want to talk about Randyl or anything? I know you really wanted to touch about mental health and PTSD and all that. I wanted to make sure that you talked about everything that you wanted to talk about there.
Randyl Nielson: Yeah. I mean, I feel we kind of covered everything.
Chris: Yeah. Your website one more time is nielsonphoto.com and then your Instagram is, what's your Instagram name? I didn't have that written.
Randyl Nielson: So the one for the cannabis is @utah.herbal.medication. And then I've got a separate one for just random photos @RandylNielsonPhoto.
Tim: Nice. Well, thanks for coming on.
Randyl Nielson: No, thank you. I appreciate it. Thank you for liking my work. It's nice to hear.
Tim: All right, everybody stay safe out there.