
Utah is similar to most other states with Medical Marijuana programs in that we maintain a list of qualifying conditions for which Qualified Medical Providers (QMPs) can recommend Medical Cannabis. The list is comparatively short when you consider how many different illnesses, injuries, and maladies people suffer with. Still, you might wonder if medical cannabis can be used for non-qualifying conditions.
The answer is not black-and-white. It has to be looked at from multiple angles, beginning with what the Compassionate Use Board (CUB) has to say about it. Then there is also the issue of obtaining a Medical Cannabis Card.
Right off the bat, you need to know that Utah law does not give patients the right to self-medicate. Qualifying condition or not, you are not allowed to grow marijuana plants in your backyard for the purposes of treating yourself. All Medical Cannabis consumed in Utah must originate from a Utah cultivator. It must be processed by a Utah processor and sold through a Utah Medical Cannabis pharmacy.
If you are using marijuana products in any unapproved way consider joining Utah’s Medical Cannabis program and make your use of cannabis legitimate. Getting a Medical Cannabis Card is no more complicated than filling out an electronic application form and visiting with a QMP.
When legislators were crafting Utah's Medical Cannabis laws, they were fully aware that there may be times when Medical Cannabis is appropriate despite a patient not being diagnosed with a qualifying condition. They created the CUB for that very reason.
If you and your doctor believe you suffer from a condition that would be well-served by Medical Cannabis despite it not being on the qualifying list, you can always petition the CUB. The CUB is a panel of seven experts given the task to approve Medical Cannabis use outside normal state rules.
The CUB routinely reviews applications from people diagnosed with non-qualifying conditions. They also review applications from minors, given that state law prohibits children from using Medical Cannabis. At any rate, your condition will generate one of three results:
In the third case, you would have 90 days from the completion date of your application to provide the additional information. The CUB would review that information and render a decision from there.
Petitioning the CUB used to involve downloading a PDF application form, completing it, and sending it to the state. That is no longer the case. The CUB now utilizes an online form. Furthermore, it is a form you would never see as a patient. Instead, your QMP completes it.
To get the ball rolling, you would apply for a Medical Cannabis Card online. You would then see a QMP with whom you would discuss your condition. If you have non-qualifying conditions, your QMP would note that on the application. Next, the state would send the QMP an invitation to fill out the CUB petition form. Then it is a matter of waiting on a decision.
Medical Cannabis can be used to treat non-qualifying conditions under certain circumstances. Ultimately though, that decision rests with the CUB.
Did you know that roughly 47.1 million Americans are living with a mental health condition of some kind in 2021? And that’s only including people with official diagnoses! For a long time, your only (legal) options for treating mental health conditions were harsh prescriptions and therapy. While these are good and necessary options for some, they aren't for everyone. Luckily, the medical community has begun to embrace the possibility of cannabis medicine positively affecting a person’s mental health. At KindlyMD, our affiliated clinic, we see patients every single day that tell us how much happier they are after switching to Medical Cannabis, and some of them have even agreed to share their stories with us on the Utah in the Weeds podcast, hosted by our founder, Tim Pickett. If you’re no stranger to poor mental health, you know how easy it is to feel alone and helpless at times. I promise you're not. Here are just a few of the success stories shared on the podcast about using cannabis for mental health conditions.
 Use Medical Cannabis for PTSD, like Vanessa & Randyl
Use Medical Cannabis for PTSD, like Vanessa & Randyl"I’ve been diagnosed with PTSD three different times over 25 years. The first one was when my husband was killed by a drunk driver. I had a lot of really weird situations. Anyways, neither here nor there, I think that I self-medicated all those years because I couldn’t take antidepressants and I didn’t want to be wiped on Valium or Xanax. I had a full-time job, I had a kid to raise, didn’t have time to mess around. I’ve always paid my own bills, always been super responsible. So, it’s hard to admit back then that I was that heavy of a pot user because people would judge me and be like, 'Oh.' But if you didn’t know me and you met me, you’d never guess now, would you?”
"With the PTSD/bipolar combo, sometimes you just don’t know what the hell you’re going to find when you wake up. You can be happy and having a good day and you wake up the next day and it’s going to be three or four weeks of pure hell of being miserable and depressed, or even worse getting into a mixed episode where your anxiety is amped up. And cannabis is essential in calming me down. The way that I used to describe it to my wife before she got her Med Card and got her to understand. How it works is: it’s like a nerve blanket. So it’s my nerves are just fried, they’re frazzled, they’re raw. And it’s like somebody just put a blanket around those nerves and just calmed them down and helped me relax."
"I was on SSRIs, I was on anti-anxiety medication, I was on sleep medication, I was all sorts of pharmaceuticals and the most unhappy I’ve ever been. So for me, it was like, 'I’ll just use it at night. I’ll just use it for sleep. And if I break a tooth, then I have it for pain.' So that’s what I qualified under. And it wasn’t until I started experimenting — because I tried the flower, I tried the capsules, I tried the tinctures, I tried the stuff you rub on your jaw, like the balms, I tried the vape. I tried all of it — and that’s when I noticed, 'Holy shit, this is actually helping my anxiety. I wonder what would happen if I used it for a panic attack.' And so I would try it that way. And I think that’s when I was like, 'Oh my God, this isn’t just a party drug.' There are so many different things that this is helping with."
"(Cannabis) helps more than any of the ADHD medications I’ve ever been on either. It helps with my anxiety more than all of those drugs. It helps with my ADHD, PTSD, my pain. It really helps in a better way than all of them."
"I suffer from PTSD — and when I say PTSD I really just mean I suffer from the nightmares of war that haunt me — and in order to put them to bed, I smoke Indica so I can sleep. I don’t want to dream, and I prefer that way, way, way over what I had chosen previously, which was alcohol."
"Sometimes I’ll close my eyes, I’ll stop to relax, and then I’ll get a flashback of something, and it’ll just make me uncomfortable and I’ll cringe, and I just get really anxious. And depending on the flashback and the severity of that situation, there are some nights where I just can’t sleep, period. With cannabis, if I have a higher dose edible, that’s the biggest part. That’s the biggest help for me, is being able to fall asleep, stay asleep, not have any nightmares. Usually, I have really great dreams or no dreams at all, and I’m just out."
While Medical Cannabis isn't the answer for everyone, we want you to know there are alternatives out there. Keep in mind that in Utah, PTSD is the only approved qualifying mental health condition for Medical Cannabis use. However, many of the patients we see at KindlyMD for other qualifying conditions find that their canna-medicine treats more than what they had bargained for. Take a quick, confidential prescreen to see if/how you qualify for Medical Cannabis in Utah, or give us a call to chat about your options. (Note: always be open and honest about your cannabis use with each of your medical providers. Cannabis & mental health medications may interact poorly.) And remember, you are not alone in this.
Catch full episodes of Utah in the Weeds here, on Spotify, Apple Podcasts, or anywhere else you listen to podcasts.
If you are in crisis or you think you may have an emergency, call your doctor or 911 immediately. If you're having suicidal thoughts, call 1-800-273-TALK (8255) to talk to a skilled, trained counselor at a crisis center in your area at any time (National Suicide Prevention Lifeline). For those located outside the United States, call your local emergency line immediately.
If you had to explain the Medical Cannabis Card to a friend or family member who had never heard of it before, what would you say? Explaining that the card allows patients to legally buy Medical Marijuana products would be a good start. But did you know that the state issues five different types of Medical Cannabis cards?
It's true. The five different types of Utah Medical Marijuana Cards are aimed at a different demographic. Between all five, the state covers adult patients, minors, and out-of-state visitors.
The standard card we tend to think of most often is what the state refers to as the 'Patient Card'. It is issued to all qualifying adults who are at least 18 years of age and have the ability to obtain their medicines on their own.
Next up is the Guardian card. It is issued to either the parents or legal guardians of eligible minors. For instance, if you have a minor child suffering from epilepsy, your child's doctor might determine that Medical Cannabis is the best option for controlling seizures. You could be issued a Guardian Card that allows you to buy medication on behalf of your child.
The state website says that Guardian Cards are issued in conjunction with Provisional Patient Cards. The Provisional Cards go to minors under the age of eighteen who are eligible to use Medical Marijuana. In essence, both of the minor child and parent or guardian get a card.
It's not as easy to get a Provisional Card compared to a standard Patient Card. That's because state law mandates that Provisional Card applications be reviewed by the state’s Compassionate Use Board prior to approval.
For the record, the state isn't purposely trying to discriminate against minors. The rules were enacted based on studies that show certain risks among minors who use Medical Marijuana. They just want to be sure that approval is in a child's best interests.
There are adult patients who, for one reason or another, are unable to obtain their medicines independently. They still qualify for Medical Cannabis under state law, but they need another adult to make their purchases. Those other adults are given Caregiver Cards.
The patients themselves get Patient Cards as well, and they must specifically designate those caregivers they want to obtain medicines on their behalf.
Finally, the state recognizes that Medical Marijuana users from out-of-state visit Utah from time to time. In order to help such visitors avoid violating federal laws by transporting marijuana products across state lines, the state issues non-Utah Resident Cards on a temporary basis.
Out-of-state visitors with valid Medical Cannabis Cards from their own states can apply for the 'visitor card' in advance of their scheduled travel dates. However, the condition for which they use the drug must be on Utah's Qualifying Condition list. Temporary visitor cards are valid for 21 days and may be applied for twice per year.
There you have it: the five types of Medical Marijuana Cards issued by Utah. If you think you or a loved one qualifies for Medical Marijuana, we would be happy to consult with you. Make an appointment at your earliest convenience to see a QMP at any one of our clinics.
A standard prescription obtained from your doctor includes instructions on dosage and delivery. Those instructions are printed on the bottle. Doctors may consult with pharmacists about modifying their original instructions as needed. Do things work the same way with Medical Cannabis in Utah? Yes and no.
First of all, the state uses specific terms to refer to medical providers and pharmacists in the Medical Cannabis arena. Medical providers (doctors, physician assistants, etc.) are known as Qualified Medical Providers (QMPs); pharmacists are known as Pharmacy Medical Providers (PMPs).
The next thing to know is that Medical Cannabis recommendations are not the same thing as traditional prescriptions. Your QMP is not required by law to write out a detailed prescription the same way they would if prescribing antibiotics.
State law allows QMPs to submit directions for dosage and delivery guidelines at the time a patient is seeking to get a first Medical Cannabis card or renew an existing card. When a QMP chooses to do so, those directions are entered into the state's electronic verification system (EVS).
Entering information into the EVS is strictly for record-keeping purposes. QMPs, PMPs, and patients are not bound to those directions in the same way they would be for another type of prescription.
What happens if your QMP doesn't submit directions for dosage and delivery? You work with your PMP on that. Note that state law requires patients to consult with a PMP at least on their first visit. In essence, you can work with your PMP to determine delivery method, dosage, the best products for your condition, etc. In fact, the state encourages you to do so. Your local PMP’s job is to help patients like you maximize the benefits of using cannabis medically.
From our point of view, it is best when the QMP and PMP work together. Your QMP best understands your medical history, and your current condition and prognosis. Your PMP adds to the QMP’s consultation by helping you find the best Medical Cannabis strains and delivery methods for your needs.
Cannabis interacts with the human body’s own endocannabinoid system, or ECS, which helps to regulate a variety of other systems within the body. Unfortunately, at many medical schools, future medical providers are given little to no education on the ECS.
Pharmacists, on the other hand, are well-versed in the ECS and how drugs like cannabis can play a role in a patient’s treatment plan.
Medical Marijuana is different from other prescription medications on multiple levels. It is different in the sense that QMPs are not required to write out detailed dosing recommendations. They can if they want to, but they can also allow PMPs to handle it.
Some medical providers aren't comfortable writing Medical Cannabis dosing recommendations due to a lack of knowledge, so we think it’s great that they’re allowed to pass that responsibility to PMPs.
Now that QMPs can leave delivery and dosage instructions to PMPs, we hope more medical providers will seek certification to become QMPs and help more Utah patients Feel Better.
The cannabis community had its own language long before states began legalizing the plant for medical purposes. But now that Medical Cannabis is a thing, that language is growing. We are hearing all sorts of terms that mean one thing to cannabis users but something completely different to everyone else. “Cannabis Layering” is just one of them.
Have you heard friends talking about layering their cannabis? Well, it turns out that the term actually has multiple meanings. Patients define it one way while growers define it another. Layering takes on its meaning depending on who you are talking to.
We think it's cool that both types of layering actually benefits patients. With that said, we've probably got you thinking whether or not it would work for you. So, to answer that question, let's discuss both types of layering.
As a Medical Cannabis patient, you probably work with your QMP and PMP to figure out your best way to consume. You talked about things like vaping and dry heating. You talk dosages, frequency, and everything in between.
If your discussions turn to layering, what you are talking about is using multiple delivery methods and dosages to achieve your goals. It is a lot like layering your clothing during those cold Utah winters. You layer as much as you need to stay warm. In terms of Medical Cannabis, you layer in whatever way provides the most relief.
Layering is based primarily on delivery methods. In Utah, regulations allow:
An example of layering might involve chronic pain and helping you sleep throughout the night. A nice tincture will help with the sleep, but it may take an hour or two to really kick in. So, in the interim, you vape a small dose to alleviate the pain so you can actually fall asleep. You are layering your medications for maximum medical benefit. Watch a video created by our founder, Tim Pickett, PA-C, that breaks down the importance of microdosing when layering cannabis.
The second type of layering is one we do not hear much about. It applies to growers looking to produce cannabis clones that are as large and healthy as they can be. Layering makes it possible to produce new plants on a live mother plant.
Growers can layer their cannabis plants in a number of ways. One of the most popular methods is known as air layering. Here, a grower is essentially scoring the healthy branch of a mother plant, then covering and fertilizing it to encourage the growth of a new branch. Once that branch is large and healthy enough, it can be cut off and planted like any other clone.
Air layering is a pretty fascinating process to observe. It turns out that cannabis growers are not the only ones who do it. Air layering is a good way to produce all sorts of fruit trees along with woody plants. It is almost like they were made to be cloned this way.
At any rate, now you know what your friends are talking about when they mention layering. In most cases, layering refers to using multiple delivery methods and varying doses to achieve the maximum benefit Medical Cannabis has to offer. When growers are talking about layering, they are referring to how they produce plant clones.
What do you think? If you are interested in layering as a patient, talk to your QMP or PMP about it. Layering may be the key to getting the kind of relief you haven't been able to get thus far.
In case you’ve been living under a rock: summer is upon us. The sun is out, temperatures are rising, and it really feels like we can get back to the good life again, doesn’t it? If like me, you plan to travel as much as you can this summer, we’ve got some tips to keep you safe if you choose/need to bring your medicine with you. If you're staying in the country, you've got quite a few options, especially if you already have a Medical Cannabis Card.
Before we get into the nitty-gritty, we've got to talk terms. When dealing with a federally illegal controlled substance like this, it’s important to know exactly what your rights are. A misjudgment of the law in your current location could land you in some pretty hot water, so let’s go over the big ones.
Recreational/Adult Use: This typically means that any person over the age of 21 can consume it, possess reasonable amounts of it, and maybe grow a plant or two. Recreational programs typically follow the same guidelines as alcohol — be wary of where you are when consuming, don’t operate heavy machinery or drive, etc. Sixteen states in the US, plus the District of Columbia, fall into this category. Many recreational states also have medical programs.
Medical/Medicinal: This means that cannabis use is approved for a (sometimes very limited) range of medical conditions. Utah falls into this category with 35 other states. Some of these states also have reciprocity laws, meaning that visiting patients with an active Medical Cannabis Card can gain access to the dispensaries, but we’ll get more into this later.
Decriminalized: Depending on the state in question, decriminalized cannabis can mean many things, but typically it means no jail time. Decriminalized states have lowered penalties for possession and use to a citation, fine, or misdemeanor. Some decriminalized states also have medical programs.
Illegal: This one is pretty self-explanatory. Don’t do it!
The easiest way to ensure you’ll have access to your medicine while traveling is to visit a place where cannabis is legal for adult use. Remember, legal doesn’t always mean legal, so it’s best to familiarize yourself with specific caveats to state recreational programs. Here are some things you’ll want to know before your trip to a recreational or adult-use state.
 however, Alaska legalized consumption on-site at dispensaries in 2019. So, if you find yourself in Alaska and need to use your medicine while you’re out, find the nearest dispensary. Alaska also has a medical program.
however, Alaska legalized consumption on-site at dispensaries in 2019. So, if you find yourself in Alaska and need to use your medicine while you’re out, find the nearest dispensary. Alaska also has a medical program.

In layman’s terms, a state with Medical Cannabis program reciprocity is a state that will honor Medical Cannabis patient status and Medical Cannabis Cards from other states, through mutual or corresponding actions. You may not get all the benefits you’d get in your home state, but you’ll get some. States that will honor a Medical Cannabis Card in some capacity are as follows:

Laws change all the time and are not standard in each state, so we always recommend looking into the laws of the specific state you plan to visit before your trip. Some states will only honor reciprocity from certain states, while others will allow you to possess during your stay, but not purchase. Know before you go.
*These states allow for reciprocity in the form of a temporary card that the medical patient must apply for. These temporary Medical Cannabis Cards are often limited to a certain number of days per calendar year. Please look into the reciprocity programs in the state you plan to visit to ensure that you qualify.
As mentioned above, “decriminalized” can mean many different things depending on where you are. States that have decriminalized cannabis have typically eliminated the threat of incarceration for possession, use, or purchase. Many decriminalized states have legalized cannabis either medically or recreationally as well, but not all of them. (Looking at you, Nebraska and North Carolina.)
Technically speaking, if a patient were VERY desperate and in need of Medical Cannabis and taking an unavoidable trip to one of these states, it’s certainly safer to consume here than, say, Idaho. We never recommend illegal use of cannabis, but if you must, make sure to look into the charges you’d face if caught. Fines will vary according to state, the amount in possession, or for repeat offenders. Say it with me this time: know before you go.
If you’re planning to visit the following states any time soon, know that any possession, use, purchase, or sale of cannabis in any form is absolutely prohibited. If caught doing any of those things, a patient faces fines, jail time, or felony charges.
I feel obligated to remind all of you that I am not a lawyer. UtahMarijuana.org does not offer any official advice on this site, whether medical or legal. Saying “but this blog post said I could!” will not hold up in court. Do your research, be smart about it, and consult a legal professional for advice if needed. Please comment below with any tidbits about other states’ cannabis laws that you’ve found or a sweet reciprocity perk you’ve encountered. We'd love to hear from you. And as always, stay safe out there.
Note: We do our best to update posts like this when legislative updates are made, but may not catch everything. Please confirm laws and regulations in the state you plan to visit with state legislation.
"Laws," WeedMaps, accessed June 24, 2021, https://weedmaps.com/learn/laws-and-regulations.
What are the first three things to come to mind when you think of cannabis? Dr. Dre? Munchies? Cheech & Chong? Loads of people, places, and things have come to be associated with the plant over the years. Heck, there’s even a holiday. We’ve likely all heard of 4/20, and many of us have even celebrated the cannabis-themed holiday at one time or another. (4/20 blaze it!) 4/20 can really refer to anything cannabis-themed. It’s a day to celebrate, a time to celebrate, and a secret code to talk about cannabis in public. (Though, at this point, it's more of a wink to cannabis use than a code.) But where did it come from? How did the tradition start and how in the world did we land on the number 420? Here are some popular theories.
Perhaps the most credible story of the history of 4/20 traces back to 1971 in Marin County, California. Five students would regularly meet at 4:20 p.m. to partake in cannabis near a statue of Louis Pasteur on campus. The time was chosen simply by convenience, as their extracurricular activities ended just before then. These students became known as “the Waldos,” a nickname that stemmed from the wall they'd lean on while smoking next to Mr. Pasteur. They began to refer to smoking as “420ing” so as to not arouse suspicion and would salute each other in the halls with “420 Louis!” The “Louis” was dropped somewhere along the way.
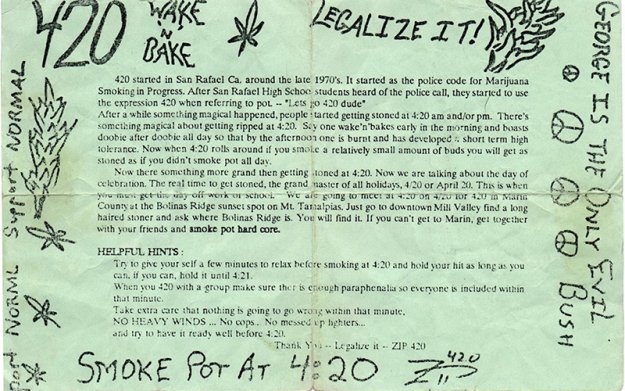
Years later, a member of the Waldos went on to work as a roadie for Grateful Dead bassist Phil Lesh, where the band helped them bring “420” to the masses and popularize the term. At a Grateful Dead show in December 1990, a group of Deadheads passed out flyers to invite people to “smoke 420 on April 20th at 4:20 p.m.” (Actual flyer pictured right.) After that, the term began to spread like wildfire.
Like any good legend, the Grateful Dead story is disputed. (Though, the Waldos have some dated memorabilia to support their story.) There are people out there who are adamant that the term 420 stems from the Bob Dylan song “Rainy Day Women #12 & 35,” as 12x35 = 420. The song also features the lyric “Everybody must get stoned” in its chorus. Seems possible!
If you're like me, somebody told you when you were young that people smoke weed on 4/20 because that was Adolf Hitler’s birthday. There was some morbid story about hotboxing … regardless, there’s been no direct link from 4/20 to Hitler. It's also been said that there are 420 different compounds in cannabis, but this isn't the case either. The actual number of compounds is highly debated, but it's not exactly 420.
Others swear that 420 comes from the old California police code for unlawful possession of marijuana. Some say it's a penal code for marijuana use. Turns out, it's neither. "But what about California State Bill 420?" you might say. It's true this bill refers to Medical Marijuana use, but the bill was named after the term, not the other way around. This was just California being a little cheeky with us.
To many these days, 4/20 is just as much a holiday as Halloween or Easter. You can attend community events all over the world to celebrate High Holiday. Many cities hold a yearly Cannabis Cup on April 20th, where hundreds of vendors can show off all their fine cannabis products or even catch a performance from such artists as 2 Chainz or Snoop Dogg, if they’re lucky. In addition to the possibility of winning the Cannabis Cup, attendees can participate in many other fun activities, such as comedy shows, marijuana-friendly speed dating, or glassware trade shows. (That's bongs, pipes, dab rigs, etc.)
If crowds and festivals aren’t your thing, don't write off 4/20 just yet. While the holiday has become a bit commercialized in its day, that doesn't stop lovers of Kush Christmas from celebrating in a more low-key fashion without all the sponsorships and marketing. Many prefer to stay home and have a blunt (or two, or three, or four) with friends. (Remember, no blunts in Utah! Stick to vapes, gummies, tinctures, or topicals to stay legal.) Others who use medicinally see it as just another day of medicine, but use the day to be grateful. April 20th has a different meaning for everyone.
What's your favorite 4/20 origin story? Comment below, especially if you’ve heard of one not mentioned here. We love a good urban legend. And please, however you choose to celebrate 4/20, do so responsibly. Schedule to get your Med Card now if you need to make it legal. Happy holidaze.
Waxman, Olivia B. “420 History: How April 20 Became Known as 'Weed Day'.” Time. Time, April 13, 2018. https://time.com/4292844/420-april-20-marijuana-pot-holiday-history/.
Lopez, German. “4/20, The Marijuana Holiday, Explained.” Vox. Vox, April 19, 2019. https://www.vox.com/policy-and-politics/2019/4/19/18484698/what-is-420-meaning-marijuana-legalization.
Carter, Ashleigh. "What is the History of 420?" Now This News. Now This News, April 20, 2020. https://nowthisnews.com/weed/what-is-the-history-of-420.
Conradt, Stacy. "What Is the Meaning Behind "420"? Mental Floss. Mental Floss, April 20, 2018. https://www.mentalfloss.com/article/62749/what-meaning-behind-420.
It's not uncommon for Medical Cannabis patients to use terms like 'cannabis', 'marijuana', and 'hemp' interchangeably. It can easily lead to confusion. Throw in discussions on THC and CBD and things get even more confusing. There is a reason for this: people just don’t understand the terms.
An incredibly wise person once said that the key to having difficult discussions is to define your terms and avoid pronouns. Regardless though, defining the terms is important when you're talking about Medical Marijuana.
For example, cannabis and hemp are not two separate plants. Neither are hemp and marijuana. Hemp and marijuana are both species of cannabis sativa. The biggest differences between the two are the amount of THC they contain and the viability of their seeds.
Hemp and Medical Cannabis are both legally allowed in Utah. Most of the hemp grown in the state is grown for industrial use. Whether for industrial, medical, or personal use, growers have to abide by the federal THC threshold.
Federal law defines hemp as cannabis sativa plants with a THC content of 0.3% or less. This is achieved through breeding. As long as a plant's THC profile comes in under the threshold, it's fine. If it exceeds it though, it is no longer hemp – it is marijuana.
According to a 2019 article published by the Salt Lake Tribune, authorities destroyed more than 16,300 plants that year because they came in above the 0.3% limit. In the industry, this is what’s known as 'testing hot'. Licensed growers cannot grow hot plants without a separate license. And even at that, doing so is for medical applications only.
A few months ago, we published a blog post discussing the main differences between CBD and THC. Those differences mean everything when it comes to classifying Medical Cannabis products. Still, both CBD and THC are medically viable, which is to say they can both be used as medicines.
So what happens to hemp that is grown for medicinal purposes? It is sent to processors who extract the THC and CBD. These extractions are subject to the same federal threshold. Extractors who produce products with more than 0.3% THC content are now producing Medical Cannabis products.
They can do a lot more with CBD. This explains why there are so many CBD-infused products on the market. And yet those products are often confused with Medical Cannabis products because many people don't know the difference between CBD and THC.
What it really boils down to is a lack of solid education. People just don't know the terms. This is true on so many levels. From legislators to retailers and consumers, a lot of people don't clearly understand the finer points of cannabis, hemp, marijuana, THC, and CBD.
As long as the Beehive State has agreed to legalize Medical Marijuana, it's probably a good idea to follow up with a more robust educational program. Maybe it's time to start teaching this stuff in our schools. It is definitely time to begin educating doctors and pharmacists.
We've learned a lot about Medical Cannabis and hemp over the last couple of years. There is still a lot more to learn though. Education is the key. The more we know about the many benefits of the cannabis plant, the better prepared we will be to use it to our full advantage.
Cannabis has been cultivated for industrial and other purposes for thousands of years. You would think that there would be little confusion as a result. But sadly, this is not the case. People cannot properly define the terms, and until they can, there will be this confusion.
Did you catch our live Q&A session on April 1st? If you didn't, it's okay. We won't hold it against you. In fact, we recorded the whole thing for you so that you don't miss out on the education and conversation had. Watch the 90-minute video below as Tim Pickett, founder of utahmarijuana.org & Blake Smith, CSO of Zion Medicinal, discuss Medical Marijuana for mental health conditions before turning the floor over to you and taking all your burning questions. If 90 minutes is more than you can spare, don't worry. We'll be cutting this up into bite-size pieces to make it easier for you to find the information you're looking for. Subscribe to the Discover Marijuana YouTube channel to be notified when those go live.
We asked you to submit your questions early and all through the event, but we had so much fun geeking out about Medical Cannabis that we couldn't answer all of them without keeping you there overnight! (But really, how much fun would a Discover Marijuana Sleepover with Tim & Blake be?) Here are all the questions we didn't get a chance to discuss.
There are no current cultivation licenses available. Contact the Department of Agriculture —more cultivation licenses must be added to the legislature before more become available.
Yes, CBD is neuroprotective and is a mild anti-inflammatory. Combined with THC, it can decrease nerve pain. Some patients report a substantial decrease with the right dosing. We recommend ratios of 5mg CBD to 1mg THC to start, increasing the dosing to reach the desired effect. Sometimes it helps immediately, sometimes it takes a while with consistent use at low to moderate doses to see any results. Visiting with a QMP will be helpful.
Neither Blake nor Tim know of any significant data on sickle cell and cannabis. It might help with some of the pain, but no data has been released supporting the fact that it would help the underlying condition.
What a question! I do not believe you will capture the market by showing bong rips or smoking joints. We have to build trust in the system, trust in the providers, and trust in the patients as well. If we are respectful to the plant and its potential benefits, while being honest about the risks and the stigma, I think we can make headway with a lot of different cultures and populations.
There is no specific program for disabled veterans. Tim’s clinic, UTTHC, offers a discount to veterans. We also offer free consultations and checkups during your first eight months in the program. Federal law protects veteran benefits when veterans participate in a state Medical Marijuana program, so you’ve got nothing to lose.
Cannabis inhibits saliva production by stimulating the CB1 and CB2 receptors. It’s the same stimulation that occurs with Anandamide. Anandamide is the endocannabinoid that stimulates CB1 receptors. This molecule is increased with physical activity, which is why running gives you a dry mouth and makes you thirsty. It’s the same mechanism.
There are two suggestions I have. The first is to be patient, as consistent supply will come over the next 1-2 years. The second suggestion is to purchase your own CBD oil (Zion makes a great one that is available in most Utah Medical Cannabis pharmacies and all UTTHC clinic locations!). Then, purchase stronger products in the pharmacies and mix your own ratios. I guess a third suggestion would be to keep a journal about what ratios and milligrams of cannabinoids are in the products you choose. This way, when you go to the pharmacy and they do not have what you need, you can try to find something similar. Keeping a journal is always a good choice.
(Zion makes a great one that is available in most Utah Medical Cannabis pharmacies and all UTTHC clinic locations!). Then, purchase stronger products in the pharmacies and mix your own ratios. I guess a third suggestion would be to keep a journal about what ratios and milligrams of cannabinoids are in the products you choose. This way, when you go to the pharmacy and they do not have what you need, you can try to find something similar. Keeping a journal is always a good choice.
Stay tuned for an upcoming video about Delta 8 and its benefits and downfalls.
As for Tim, out-of-state businesses don’t play much into the success of his business. However, when it comes to Zion, Utah law protects them by not allowing other operators to open businesses until the law is changed. Once that law changes, there are no guarantees. Anybody who is in the cannabis business will tell you we live in a constant state of change. It can be hard to keep up.
This is a really interesting statement that ultimately points to the fact that all products and people are different. Here’s another example: in medical school, we’re taught to treat depression with one of five medications. All have the potential to help the patient. If no improvement is made in the condition in a month or so, we change the medications. We are taught to try 3-4 different medicines before changing the class of medicine (antidepressants to stimulants, for example.) The same is true for cannabis. In fact, cannabis is even more finicky. I would recommend trying a different brand, different cannabinoid ratios, different terpene profiles, different delivery methods. With care and determination, always keeping a journal, you’ll have the best chance of finding something that helps. Blake won’t take it personally if you don’t use his product. The important thing to both of us is that you feel better.
Keep an eye out for an upcoming episode about all our favorite Deltas!
Tim & Blake will be releasing a video in the near future to answer all your questions about Delta 8, Delta 9, Delta 10, etc.
There is some debatable evidence about blood thinning and cannabis use. All of the evidence, however, relates to ingested methods — inhaled or oral. We aren’t aware of any evidence that topical cannabis could cause an increase in bleeding risk. Slather it on, you should be good to go!
Once the molecules are in the bloodstream, they’re going to distribute the same. There are some complicated differences in the bioavailability of inhaled methods versus ingestibles, though. Inhaled products cross directly into the bloodstream without any metabolism or breakdown, so the bioavailability is very high and depends on the concentration of the product being inhaled. Digestion and absorption go through the liver, which changes the molecules and reduces bioavailability. Edibles can be 30 to 50% absorbed compared to inhaled methods. However, once it goes to the liver, THC can be transformed into a slightly different metabolite much stronger than THC. Therefore, edibles can sometimes cause a stronger reaction in the body, even though they are less bioavailable.
Keep an eye out for an upcoming article about this topic on the utahmarijuana.org blog. It’ll be pretty technical. Good question! Generally, no, there’s no difference in distribution and effect between delivery methods, only in the medications/product taken.
We recommend starting with a decent amount of CBD combined with THC. Sometimes adding other cannabinoids can help, depending on the individual. Fibromyalgia is one condition where keeping a journal is paramount. Keep track of what you’re taking, be consistent, and you’ll likely find something that helps you feel better over time. I would say most patients require 4-6 weeks before really dialing it in. Try to stay positive and don’t give up!
Well, the endocannabinoid system isn't fully developed until a person reaches 20-25 years old. That being said, we give our kids ibuprofen and Tylenol without batting an eye just because it’s FDA approved. Cannabinoids are naturally occurring and some amount of CBD is likely safer for all age groups. While I can’t provide specific medical advice for this question, in general, I would say trying a CBD product you trust for one or two months at low doses seems reasonable to me.
We have a handful of patients under 16 — the youngest of which is under two years old — who use CBD in low-to-moderate doses with pretty good results. Be honest about your child’s CBD use with your pediatrician or other medical providers. If you need more assistance or information, don’t hesitate to reach out and schedule an appointment with me to talk about it. We offer free phone consultations for all pediatric patients to help determine what the next steps are.
Tim & Blake can't thank you enough for your support of the Discover Marijuana educational video series. We've had so much fun creating these videos for you and bringing frank, unbiased education to the people of Utah and beyond. There's so much more Tim & Blake to come, so stay tuned! Subscribe to the Discover Marijuana YouTube channel to be the first to see new episodes, live sessions, and more educational videos about Medical Cannabis. Comment below to let us know what topics you'd like us to cover in a future episode, and subscribe to the utahmarijuana.org mailing list below to receive bonus content, invitations to events, and more.