
Think back to science class. Specifically, think about all that you learned about the endocannabinoid system (ECS) and marijuana treatment. Doesn’t take too long, does it? That’s because you probably learned about as much as I did: nothing. And I went to medical school!
Okay, so that’s not completely true. In medical school, they teach about cannabis as a drug of abuse. They also teach that it’s federally classified as a Schedule 1 drug and that “we need more research” on the benefits. It's clear to me now that what we all learned in school, from way back to grade school in many cases, needs to be discarded. It truly bears no relationship to reality.
In my opinion, “we need more research” is a cop-out. There have been thousands of studies on the plant, its side effects, dosing, compounds, and most importantly, its safety. The fact is, it's somewhat difficult to conduct research with cannabis. However, I would argue that this isn't due to its federal classification, but due to the complexity of the research that would need to be conducted.
Effective research on cannabis is similar to doing research on different tomato plants. You'd have to study the effect on different body systems depending on the type of tomato, the way it's processed, how it's cooked (or not cooked), and how it's consumed. Ketchup is useful, tasty, and goes great on hotdogs, but it’s night and day to a fresh tomato picked off the vine. The same is true for cannabis.
Israel, for example, has one of the world’s largest cannabis labs on earth. In their studies, they've found that one strain processed into one batch of tincture works to prevent seizures in one individual, while the same brand as a different batch or strain doesn't. The 113 cannabinoids (CBs) and 400 other compounds within the plant need to line up perfectly, in just the right proportions, to have the same effect.
Most medical providers didn't learn about the endocannabinoid system in medical school. We only discovered it in the 1980s, around the same time that we discovered cannabinoid receptors. In fact, all humans and complex animals have an endocannabinoid system 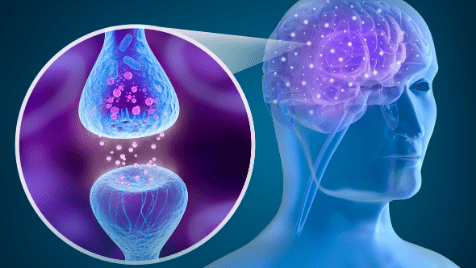 that works to maintain homeostasis. The ECS affects memory, digestion, motor function, immunity, inflammation, appetite, pain, blood pressure, bone growth, and the protection of nerve and brain tissues, just to name a few.
that works to maintain homeostasis. The ECS affects memory, digestion, motor function, immunity, inflammation, appetite, pain, blood pressure, bone growth, and the protection of nerve and brain tissues, just to name a few.
When THC binds to CB-1 receptors in your brain, you begin to feel the psychoactive effects or feel "high." Because there are very few CB-1 receptors in your brain, an overdose of cannabis won't cause breathing problems or death, as an overdose of other medications would. CB-2 receptors live in your immune system. Together, the ECS is constantly working behind the scenes to maintain balance in your body.
Now, that’s a lot of scientific jargon that may not make a lot of sense to you. Maybe it does. But if you need it broken down further, check out this Zion Medicinal educational video about the endocannabinoid system.
Western-trained medical providers have been taught that one medicine does one thing and treats one illness or symptom. Do we throw away cannabis as a viable treatment option because we don’t have years and years of research behind it?
Lucky for us, the public has made this decision for us with a resounding “Hell no!” As medical providers, we need to take a step back and see that the way we’ve been taught to treat patients has played a role in them wanting to take matters into their own hands. We’ve been pushing pills and procedures on patients for generations. This has led patients to start experimenting with alternative  treatments. Through that experimentation, they've experienced firsthand that the endocannabinoid system exists. They've seen that cannabis can and does work to treat many illnesses and health concerns. They've gone around the medical community and taken their health and treatment into their own hands. It’s time for us to get on board.
treatments. Through that experimentation, they've experienced firsthand that the endocannabinoid system exists. They've seen that cannabis can and does work to treat many illnesses and health concerns. They've gone around the medical community and taken their health and treatment into their own hands. It’s time for us to get on board.
Most importantly, remember to forget every preconceived notion you have about Medical Cannabis treatment. Find a qualified medical provider (QMP) and follow their recommendations closely to find your just-right dose. Everybody's endocannabinoid system and genetic makeup is different and requires specific dosing and delivery for a beneficial experience.
So here we are. Welcome. Medical Cannabis is legal in Utah and this is what you should know according to Tim Pickett.
How Dr. Bone and Tim met [0:33]
Comparing Medical Marijuana dosages in Florida and Utah [1:30]
Tim and Dr. Bone’s thoughts on the Utah and Florida Medical Marijuana program [10:39]
Requirements for caregivers [13:53]
Dr. Bone's thoughts on cannabis treatment for Alzheimer’s and dementia [16:20]
Dispensary limits in Florida and Utah [27:55]
The process for getting a Medical Marijuana card in Florida [31:47]
How the Florida and Utah Medical Marijuana programs handle non-qualified medical conditions [34:44]
Number of Medical Marijuana patients in Florida [41:09]
Dr. Bone’s connection to Utah [44:38]
How to connect with Dr. Bone [48:28]
Dr. Bone and Tim were connected through Shawn Hammond, the grower for Zion Pharmaceuticals (check out our interview with Shawn here.) When Tim began to get involved in the cannabis scene in Utah, Shawn encouraged Tim to reach out to Dr. Bone.
Dr. Bone, based out of West Palm Beach, Florida, is an expert in cannabis and speaks internationally on the subject.
Florida medical providers do not have patient caps. However, patients do have a daily milligram cap on THC. Clinicians can prescribe a certain number of milligrams of CBD and a certain number of milligrams of THC that the patient may purchase for 70 days.
Dr. Bone found that there are Florida patients who order as little as one to two hundred milligrams of THC a day, up to 10,000 milligrams a day.
Utah patients are restricted to 20 grams (or 20,000 milligrams) per month.
Dr. Bone believes that the Florida program provides robust options for patients. However, one of the challenges she has experienced is with seniors.
The Florida Medical Marijuana program requires either a driver’s license or Florida state photo ID. However, older seniors may not have had a driver’s license for years. Also, for seniors who are in severe pain, it can be difficult for them to get to a location where they can obtain a state ID. Utah faces the same challenge, as the EVS system requires a state ID.
One difference between the Utah and Florida Medical Marijuana programs is the amount of flower that can be possessed . Utah allows patients to obtain four ounces of flower per month, versus only two and a half ounces every 35 days in Florida.
Another difference between the two states is how they handle out-of-state Medical Marijuana cards. In Florida, you must meet all residency, ID, and health qualification requirements to obtain a card, even if you have obtained a card in another state. This is especially problematic for seasonal residents, who may not have a permanent residence in the state.
In Utah, out-of-state Medical Marijuana cards cannot be used. However, a temporary card may be issued with an out-of-state license.
In Florida, every caregiver has to register and pay an annual fee to be able to administer Medical Marijuana for their patients. They also have to complete a course and pass a five-question quiz, which can be intimidating to some people.
These hurdles were created in Florida to prevent anyone from claiming they are a caregiver so that they can easily obtain Medical Marijuana.
This caregiver issue is very similar in Utah. In Utah, anyone under 21 who uses Medical Marijuana must have a caregiver. Caregivers are required to pay an additional fee and have a background check.
Dr. Bone works in a memory care unit, a locked unit for patients with all types of dementia, including later-stage dementia. Because the unit is funded with healthcare dollars from Medicare and Medicaid, they are unable to treat patients with THC products. They are able to see some success with CBD for anxiety, hyperactivity, agitation, and combative behavior. However, she also sees success with her private practice patients that are prescribed THC.
Her approach with THC and dementia is to start with a full spectrum or low THC product and assess the results. Then, if necessary, she will increase dosages and CBD/THC ratios until the patient sees results.
There are no dispensary limits in Florida. However, it is very expensive to start a dispensary. This is because dispensaries require “full vertical integration”, which means you have to grow cannabis, harvest it, process it, package it, and bottle it in your retail facilities. Dr. Bone estimates that dispensaries will require an investment of up to $60 million to get started.
In Utah, there are eight grow licenses and 14 dispensary licenses. Unlike Florida, Utah dispensaries are not required to also grow their own product. This allows growers and dispensaries to focus on what they do best.
In Florida, patients must have a face-to-face consultation and physical examination with a medical provider. This requirement was not waived during the COVID-19 pandemic.
There are no specific parameters for what the physical examination consists of. Providers are just required to provide a basic examination and review the patient’s medical history.
If the patient has one of the 12 qualified medical conditions, they can be given a Medical Marijuana card. After approval, it typically takes 14 days for them to receive a card.
The patient’s medical marijuana certification is good for 70 days. Providers can set this to automatically re-certify after 70 days. However, providers in Florida are required to see the patient every 210 days.
In Florida, patients applying for Medical Marijuana use with a non-qualified medical condition requires a letter to the state in which the physician says why the patient would benefit from cannabis, documented with medical literature to support their opinion (called a “similar diagnosis”). For example, anxiety is not an approved diagnosis. A provider would have to say it is “similar” to PTSD, which is an approved diagnosis.
In Utah, applications for Medical Marijuana use with a non-qualified medical condition require approval from the state’s Compassionate Use Board, a board of seven physicians.
As of the recording of this podcast, Dr. Bone believes there are ~400,000 patients in Florida.
Dr. Bone’s child went to an outdoor wilderness therapy program in the Uinta mountains in Utah. Her other connection to the state is as a breast cancer survivor and speaker. Specifically, she spoke on behalf of Myriad Genetics -- a company in Utah.
You can learn more about Dr. Bone on her website, drmelaniebone.com. On the site, you can contact Dr. Bone and learn more about her mentoring program for doctors.
Who is Weldon Angelos? [0:56]
Weldon’s trial and sentence [06:41]
Efforts to change Weldon’s prison sentence [8:26]
Weldon’s experience in prison [09:18]
How Weldon was able to have his sentence commuted [10:51]
Weldon’s life after prison [12:24]
Weldon’s efforts to help others in prison [14:03]
Why the Mission Green project is focused on federal prisoners [19:02]
Mission Green’s cannabis brand [21:57]
Adjusting to life after prison [22:45]
More about the documentary [24:29]
Weldon’s thoughts on medical vs. recreational marijuana [29:42]
The Weldon Project’s work to have rap artist Loon released from prison [35:02]
Weldon’s day to day life [36:43]
How Weldon learned the laws around cannabis [37:59]
How you can get involved with the Weldon Project & Mission Green [42:18]
Weldon has a background in music production, working with artists such as Snoop Dogg and Tupac. Weldon also was involved in bringing rap artists on tour to Salt Lake City.
As Weldon became more popular in the area, the Salt Lake City Metro Gang Unit began to take notice and investigated him. It was determined later that law enforcement was concerned with Weldon efforts to promote cannabis and urban culture in Utah. They were worried about “moral corruption.” An arrest of Weldon would also look good on the records of those law enforcement officials and help them get promoted.
A childhood acquaintance of Weldon became an informant for the Metro Gang Unit. Weldon gave the informant $300 worth of cannabis on three different occasions. The prosecutor on his case was able to turn these three transactions into a 20 count federal indictment with a minimum of 105 years in prison if convicted on all counts.
The prosecutor introduced evidence from Weldon’s work in music and clothing to make a case. For example, in the closing argument, the prosecutor used lyrics from an album he produced to describe his character, even though he did not write the lyrics. The prosecutor also used Snoop Dogg’s clothing line, East Side LBC, as evidence of gang affiliation.
Ultimately, Weldon was sentenced to 55 years in prison.
Before sentencing, the judge for Weldon’s trial asked President George W. Bush to commute the sentence. He believed that the mandatory sentencing he was required to impose was cruel, unjust, and irrational. However, this effort was unsuccessful. Thus, the judge was forced to sentence Weldon to 55 years without parole in federal prison.
A young prosecutor named Mike Lee disagreed with the way his colleagues treated Weldon. A few years later, Mike Lee (R-Utah) became a U.S. Senator. He did not forget Weldon, and introduced legislation to fix his sentence.
At 24 years old, Weldon was sent to the United States Penitentiary, Lompoc in California. USP Lompoc is a medium security prison for male inmates. He served his prison sentence alongside violent criminals, murders and “lifers.”
Requests for appeals were denied, so his only hope for getting out of prison was clemency from President Bush. He believed that President Bush would likely not grant him clemency, so he and his team focused their efforts on the next president, Barack Obama.
Weldon and his team were able to build a coalition of celebrities and politicians to help get his sentence commuted, including Snoop Dogg, Alicia Keys, Bonnie Raitt, Mike Epps, and Senators Mike Lee, Rand Paul, and Cory Booker.
Later, the Koch Brothers joined the effort to get Weldon’s sentence commuted, which was a shock to him and his team. The judge who presided over Weldon’s trial also stepped down from a lifetime appointment and became his advocate.
A petition was sent to President Obama that included signatures from over 150 lawmakers, including judges, former federal prosecutors, former U.S. Attorney Janet Reno, and many other former U.S. attorneys.
Finally, on May 31, 2016, Weldon was released from federal prison.
As soon as Weldon was released from prison, he hit the ground running to work on criminal justice reform. He was part of the coalition lobbying for the First Step Act, which was legislation to “improve criminal justice outcomes, as well as to reduce the size of the federal prison population while also creating mechanisms to maintain public safety.” The legislation was signed into law by President Trump in 2018.
Senators Mike Lee and Cory Booker used Weldon’s story on the Senate floor as an example of why we need to change the system. In fact, one of the provisions in the act is named after him.
The First Step Act was a great step towards criminal justice reform, but the act did not apply to purely cannabis cases.
Weldon’s tells the story of Luke Scarmazzo and Ricardo Montes, California dispensary operators who were convicted in federal court under a “kingpin” statute. They were arrested after Luke created a satire video saying “[expletive] the FEDs!”
Medical Marijuana was legalized in California at the time. However, because federal law still classifies cannabis as a Schedule 1 drug, federal officials were still able to arrest and prosecute them.
President Obama did commute the sentence of Ricardo Montes. However, he denied Luke’s request.
Weldon met Luke when they were in prison. When Weldon’s sentence was commuted, Luke asked Weldon not to forget about him.
To help Luke and others like him, Weldon is launching an initiative called Mission Green, uniting the entertainment industry with those in the cannabis industry who can help fund this initiative.
Weldon is working with White House Advisor Jared Kushner, former governor Gary Johnson, NBA Hall of Famer Kevin Garnett, and others to help get people like Luke out of prison who are in the federal system for cannabis offenses.
Unlike the state penitentiary system where there is the option of parole or even expungement as state laws change, in the federal system there is no relief unless the President of the United States commutes your sentence or Congress acts to change federal laws.
Thus, low-level drug offenses or cases in states that have legalized possession of marijuana still have significant minimum mandatory sentences.
Mission Green’s goal is to have more cases like Luke Scarmazzo commuted, putting pressure on Congress to change laws.
Mission Green is launching a cannabis brand called REEForm. The goal of this brand is to give the proceeds from sales to cannabis federal prisoner commissary accounts.
REEForm is in partnership with one of the biggest packaging companies in the country called Kush Supply Co. They are providing packaging at near cost and on credit, which will help REEForm grow nationally.
Weldon’s criminal justice reform work was a good distraction for him after prison. In his final months in prison, he knew he would be released, but did not know the date. When he finally was released, he asked friends and family to keep it a secret to give him a few days to get some sun, buy new clothes, and re-adjust to life.
Eventually, a story ran in the Washington Post that announced his release to the world. This sparked weeks of phone calls from the press and requests for him to speak around the country.
Instead of becoming bitter or returning to music, Weldon decided to use this platform to push for criminal justice reform. He is also working on a documentary and movie deal.
The documentary will be a 90 minute feature film. Weldon is currently in discussions with HBO for the project.
The documentary is produced by NBA Hall of Famer Kevin Garnett and Mark Wahlberg, and will feature Snoop Dogg, TI, President Trump, former U.S. Attorney General Jeff Sessions, and more.
Weldon believes that everyone should have access to cannabis. Weldon also believes that home grow should also be an option for cannabis users.
He would like to see cannabis deregulated at the federal level and left up to the states to regulate, similar to how alcohol is regulated.
Weldon believes in working in a bi-partisan way to improve legislation. He has worked on both sides of the aisle, including with President Trump, White House Advisor Jared Kushner, and Senators Cory Booker, and Mike Lee.
The Weldon Project is working with the federal system to have the rap artist Loon released from prison.
Update since this podcast was released: Loon was released from prison on July 29.
Weldon spends his days writing legal briefs for people in prison for cannabis, working on his cannabis brand, and networking. He continues to advocate for people in prison, male and female.
While in prison, Weldon spent much of his time studying law. With the help of his sister, he used this knowledge to campaign for his release from prison.
You can go to TheWeldonProject.org to donate or volunteer.
We have had legal Medical Marijuana in Utah for a while now. In that time, we've definitely had some ups and downs within the program. It's clear now that finding a Qualified Medical Provider with a good customer service team behind them is important. Any Medical Cannabis patient can tell you that navigating the state website and legal requirements can be a challenging feat.
In 2020, once you had seen a QMP, you received a letter of recommendation to use Medical Cannabis and were able to register that letter with one pharmacy. Many Utah Medical Cannabis patients held on to their letter for the year and didn't worry about getting their card until absolutely necessary. If you're interested, I had written an article to help educate Medical Cannabis patients about getting their letter converted to a card to gain access to more pharmacies in Utah and stay current in the program. Letters are no longer a part of the Utah Medical Cannabis program, so it's not relevant anymore, but still an interesting read.
If you're still wondering how to get started, watch this short video about how to get your Medical Card on our homepage. Now, let’s say you have your Medical Cannabis Card and want to know the process over the next few years. Settle in, and let's navigate the first two years together.
On January 3, 2021, the Utah Department of Health began issuing Medical Cannabis cards with expiration dates of six months after the patient's initial consultation.
Before then, new Medical Cannabis patients needed to have a follow-up visit with a QMP after 90 days. Although the 90-day expiration date has changed to six months, I still recommend visiting with a QMP after 90 days. That's why Utah Therapeutic Health Center continues to offer 90-day visits at no cost for our patients.
This is best practice. Nobody starts new cholesterol medication without keeping their provider in the loop on the experience and effectiveness of the medication. Medical Marijuana is no different. Your provider needs to know how cannabis use has affected you and your condition.

Just before your initial Medical Cannabis Card expires, our Patient Experience team reaches out to you by phone. We double-check the accuracy of the health information in your file, answer questions, request dosing changes from your provider on your behalf, and walk you through the renewal process on the EVS website.
The card you get after this first renewal is valid for six months. So, you'd think that now you don’t need to see your provider again for another six months, right? Wrong. State law, Medical Cannabis best practice, and national guidelines require medical providers to physically see their Medical Cannabis patients twice a year, or every six months. This usually will not match up with their card expiration date. Why the discrepancy? I wish we knew. Call it growing pains.
About six months, you’ll need to schedule a follow-up visit with your provider. While you must meet face-to-face with your provider for your initial visit, you can do your follow-up with a telemedicine visit if your provider offers that. Good news: Utah Therapeutic Health Center does! Please note that telemedicine visits are subject to availability and are offered under limited circumstances. Call us at 801-851-5554 to ask about arranging a telemedicine visit.
Providers usually charge for this six-month visit, just like going in for a check-up with your family doctor.
 During your follow-up visit, we’ll discuss new medications and health history and check up on your therapy. We’ll answer any questions you have and go over the products you have tried to ensure you're using them appropriately. We also use these visits to educate patients on Utah law, changes to the program, and changes to EVS.
During your follow-up visit, we’ll discuss new medications and health history and check up on your therapy. We’ll answer any questions you have and go over the products you have tried to ensure you're using them appropriately. We also use these visits to educate patients on Utah law, changes to the program, and changes to EVS.
If you have already seen a QMP when your expiration date nears, this can be done by phone and without additional fees. If the expiration date coincides with the six-month visit, all of these things can be done together. After this update, the card will be valid for another six months. This brings the total time to about one year from the initial evaluation and recommendation.
About 12 months after the first time you see your QMP, you’ll need to see them again by telemedicine or in person. At the one-year visit, your pathway can change depending on how your Medical Cannabis treatment has progressed. After the first year of Medical Cannabis treatment, you can go one year between visits with your provider’s approval. It is completely up to your QMP how often you are seen after the first year. In my opinion, patients should be seen at an interval of six months. That being said, from a financial and safety standpoint, many patients of our clinic will likely be approved to go one year between visits.
 Say that your QMP offers you a one-year timeline. Once renewed, your profile will reflect this and your Medical Cannabis Card won't expire for a full year. Dosing and delivery changes will need QMP approval, and that may require another visit. No dosing or delivery changes for you? Then simply enjoy 365 days of program participation! If nothing major changes and your Medical Cannabis treatment has been stable up to this point, then you will carry on as usual. Your dosage limit will renew every 28 days until you see your provider the following year.
Say that your QMP offers you a one-year timeline. Once renewed, your profile will reflect this and your Medical Cannabis Card won't expire for a full year. Dosing and delivery changes will need QMP approval, and that may require another visit. No dosing or delivery changes for you? Then simply enjoy 365 days of program participation! If nothing major changes and your Medical Cannabis treatment has been stable up to this point, then you will carry on as usual. Your dosage limit will renew every 28 days until you see your provider the following year.
Whether or not your provider recommends six-month or one-year follow-up visits depends on many factors, like dosing, medical history, medications, and best practice. Yes, certain patients and conditions require more frequent visits. We know that it can get expensive to see your provider every six months without insurance coverage, but if your health and safety depend on it, isn’t that worth it?
Please comment below with any questions you have about the first two years of the Utah Medical Cannabis program.
*regularly updated for accuracy*
In late August 2020, there were a total of 9,048 active Medical Cannabis Cards in the state, with 13,075 applications submitted. This means at least 4,027 Medical Cannabis Letters have not been converted to Medical Marijuana Cards. The estimated number of letters registered at dispensaries is anywhere from 6,500 to over 10,000, according to the Utah Cannabis Association and others in the industry.

An adjustment made to the Utah Medical Cannabis Act, passed by Utah Legislature in March 2020, allowed Medical Cannabis patients in Utah to use a letter of recommendation from any licensed medical provider in Utah to purchase Medical Marijuana in Utah's dispensaries. At the time, there were only one or two Medical Cannabis pharmacies planning to open in the summer of 2020.
Here's the issue: patients are able to use their Medical Cannabis Letter at only one pharmacy. After registering that letter with the first pharmacy they go to, they can't buy Medical Marijuana from any other, despite the fact that limited availability is a serious problem right now in Utah. Patients must register with the Department of Health to get a state-issued Medical Cannabis Card in order to purchase from multiple pharmacies.
Since March 1, only four Medical Cannabis pharmacies have opened in Utah to serve patients in Salt Lake City, Bountiful, Ogden, and Logan. A fifth, Deseret Wellness, plans to open in Provo in late August. With all of these patients in the program limited to only one pharmacy, additional pharmacies are likely hesitant to open.
 Medical Cannabis Letters will expire December 31st of this year. Any patient not holding a state-issued Medical Cannabis Card won't be able to buy Medical Marijuana at any Medical Cannabis pharmacy in Utah after January 1, 2021. Those letters must be converted into Medical Cannabis Cards before the end of the year for those patients to have access to their medicine.
Medical Cannabis Letters will expire December 31st of this year. Any patient not holding a state-issued Medical Cannabis Card won't be able to buy Medical Marijuana at any Medical Cannabis pharmacy in Utah after January 1, 2021. Those letters must be converted into Medical Cannabis Cards before the end of the year for those patients to have access to their medicine.
UtahMarijuana.org has been in discussions with leadership at the Department of Health and the Utah Cannabis Association about how to best handle this looming issue creeping up on us. Imagine 10,000 legal Medical Cannabis patients in Utah not being able to buy their medicine in January. This on top of the problems we've had with the EVS system so far! Needless to say, December, January, and February could be awful months for Utah's Medical Cannabis program, just when patients will need to have access. Remember, health officials think COVID-19 will only get worse this winter.
Patients under 21 are in an even stickier situation. As of now, patients under 21 with a Utah Medical Cannabis Letter can purchase Medical Marijuana without a guardian and without approval from the state's Compassionate Use Board. However, when the clock strikes twelve on New Year's Eve, that all ends.
Starting in January, anyone under 21 years old will need to have a state-issued Medical Cannabis Card as well as a guardian holding a guardian card to enter the dispensaries and purchase Medical Marijuana. The process for those under 21 to get their Medical Cannabis Card can take one to three months. The process requires documenting the patient's medical history with supporting records and an application completed by their QMP. Then, the patient's case is presented to the seven physicians on the Compassionate Use Board for approval. Right now, this board only meets monthly, so time is truly running out for those who need this extra approval for use.
 Granted, applying a Band-Aid that allowed Utah patients to use a letter of recommendation at one pharmacy until the end of 2020 was a good idea at the time and did give patients access to Medical Marijuana faster. However, it kicked the can down the road and created yet another potential hiccup in the Utah Medical Cannabis program that we are all going to have to face soon enough.
Granted, applying a Band-Aid that allowed Utah patients to use a letter of recommendation at one pharmacy until the end of 2020 was a good idea at the time and did give patients access to Medical Marijuana faster. However, it kicked the can down the road and created yet another potential hiccup in the Utah Medical Cannabis program that we are all going to have to face soon enough.
Just the other day, a patient mentioned to me that their QMP charged them for the initial visit and now, two months later, wants another $165 to certify them on EVS. This is unethical. Patients should not be charged anything extra to convert their Medical Marijuana Letter to a Card or for their QMP to certify them. That should simply be a given.
 UtahMarijuana.org is rolling out a program to help patients convert their Medical Cannabis letters to cards FOR FREE. We'll gather patient information and speak with the Utah Department of Health to determine where the patient is in the registration process. We'll also reach out to their medical provider to offer help and education. Yes, this is time consuming and takes an army of dedicated patient experience representatives. Luckily, we have that dedicated team on our staff.
UtahMarijuana.org is rolling out a program to help patients convert their Medical Cannabis letters to cards FOR FREE. We'll gather patient information and speak with the Utah Department of Health to determine where the patient is in the registration process. We'll also reach out to their medical provider to offer help and education. Yes, this is time consuming and takes an army of dedicated patient experience representatives. Luckily, we have that dedicated team on our staff.
We've been working with local QMPs to help them navigate the EVS system. We're also helping patients all over the state register with the Utah Department of Health. Our relationship with the Department of Health, local Medical Cannabis pharmacies, and many clinic operations within the state has given us the best pathway for patients to convert their Medical Marijuana letters into cards.
So, if you have a Medical Cannabis Letter in Utah, call or text us at 801-851-5554 extension 3 or learn more about how to turn your Utah Medical Cannabis Letter into a Card. Let us help! Reach out today and don't worry about the bottleneck of thousands of patients scrambling to get their Medical Cannabis Cards as we inch closer to Christmas.
Who is Dr. Corey Anden? [00:51]
Dr. Anden’s thoughts on smoking vs. other methods of consuming Medical Marijuana [04:49]
Dr. Anden’s thought on the current Medical Marijuana laws [9:53]
How does Dr. Anden approaches patient wellness? [13:49]
How has the COVID-19 pandemic affected Dr. Anden’s practice? [25:21]
How Dr. Anden discusses Medical Marijuana treatments for pain with patients [26:18]
Conditions that Dr. Anden would like to see as a qualifying condition [31:38]
Does Dr. Anden provide Medical Marijuana recommendations? [34:43]
Why do patients still visit Dr. Anden even though she has met her patient cap for cards? [38:42]
How to contact Dr. Anden [43:45]
Dr. Anden is a pain physician in Ogden, Utah. She also practices cannabis medicine. In fact, she has likely practiced longer than any other provider in Utah.
Dr. Anden has always been interested in cannabis. She grew up a child of the sixties and seventies in southwestern Pennsylvania.
As an adult, she became interested and fascinated with the benefits of Medical Marijuana, and began to educate herself with books and information online.
After the state legislature approved HB 3001, she focused more on re-educating patients on other ways of using cannabis for better medicinal benefits, as well as how to be compliant with the Utah laws.
Many patients are used to consuming cannabis by combustion. Dr. Anden believes that this method does seem to have benefits. However, she sees combustion as more suited for recreational use.
The chemicals in the plants and their activation or boiling points are at much lower temperatures, more in the 300 or 450 degree Fahrenheit range. In her opinion, smoking cannabis at a high temperature burns up certain cannabinoids and most of the terpenes.
Using a dry herb vaporizer would help retain the medicinal properties of the cannabinoids and terpenes by lowering the temperature to the 300 or 450 degree range.
Also, by consuming cannabis at a lower temperature, you’ll avoid the toxins, the potential carcinogens in smoke, etc.
Dr. Anden’s biggest issue with the current legislation is the patient cap. Currently, Utah law sets the patient cap at 600 patients per physician and 275 patients per PA or nurse practitioner. For medical providers who are pursuing further education, this cap limits what they can do.
She believes it is also a disservice to the patients who want to see clinicians who are experts. For example, if patients want to visit Dr. Anden because of her expertise with Medical Cannabis (she is currently enrolled in a Medical Cannabis Master’s program at the University of Maryland), traditional medicine, and integrative medicine, the law will prohibit her from helping them obtain a card. Patients can still see Dr. Anden for a consultation. However, they would need to go elsewhere for a Medical Marijuana Card.
Dr. Anden has worked as an interventional pain physician and is board certified in physical medicine and rehabilitation, pain, sports medicine, and electrodiagnostic medicine
Instead of just prescribing patients more pharmaceuticals and surgeries, Dr. Anden is passionate about the concept of a more organic approach to wellness, including cannabis medicine, healthy diet, healthy lifestyles, and healthy exercise.
She is not opposed to prescribing pharmaceuticals, including some degree of opioids. However, Dr. Anden will also consult with patients on the importance of losing weight, healthy diets, exercise, and a healthy lifestyle.
Even with the patient gap, she will still bring up cannabis and CBD as a potential treatment. With CBD, she will discuss the anti-inflammatory, anti-anxiety, muscle relaxing, immuno-protective, neuro-protective effects. If a patient then asks about cannabis, she can give them education and tailor particular medication recommendations to their diseases or disorders. However, she’ll explain to them that they will need to go to another provider for a Medical Marijuana Card.
Other than shutting down for the first two weeks of the pandemic, the COVID-19 pandemic has not affected her practice. The hospital where her office is located has implemented all of the protocols for patients, including temperature checks and a questionnaire upon entering.
For Dr. Anden, it depends on the perspective of the patient. Some of her patients have already been using cannabis and some people are new to it. Her patients may have already had multiple surgeries or have been using opioids to manage pain.
After understanding the patient's perspective and history, she will explain how the numerous chemicals, cannabinoids, such as CBD, and terpenes that can help manage their pain.
Although most patients are interested in using Medical Marjiuana to manage pain, Dr. Anden would like to see anxiety, mood disorders, and sleep disorders included as qualifying conditions.
Dr. Anden does provide specific Medical Marijuana recommendations to patients. In fact, she will review their local pharmacy’s menu and provide recommendations based on what the pharmacy offers. Patients can also call Dr. Anden for help with dosing at any time.
Often, patients will visit Dr. Anden if they are looking for more Medical Cannabis education. Patients visit Dr. Anden with conditions such as MS, Parkinson's disease, chronic pain, etc. They have tried everything and are now considering turning to Medical Cannabis for help. However, they need some guidance, so they visit Dr. Anden for help.
Dr. Anden’s website is CoreyAndenMD.com. You can also call her office at (801) 732-5914.
For more information on obtaining a Medical Marijuana Card, schedule an appointment with us today.
What types of Medical Cannabis legal issues does J.D. see regularly? [02:28]
Utah state laws about guns and cannabis [04:59]
Can the federal government arrest Medical Marijuana Card holders? [09:34]
J.D.’s recommendations for dealing with police if you are pulled over [11:17]
More of J.D.’s thoughts on the chemical test administered for DUI arrests [14:16]
Is it legal to possess and use cannabis here regardless of where you got it from? [17:30]
What is the best way to store cannabis? [19:47]
J.D. thoughts on the provisions that prevent patients from using combustion when consuming Medical Marijuana [23:14]
How much Medical Marijuana can you possess? [27:51]
Can a patient buy Medical Marijuana products from another patient? [41:06]
How to get in touch with J.D. [47:09]
Christianson and Jensen website
@utcannabislaw on Twitter
J.D. Lauritzen is a lawyer with Christensen & Jensen. J.D. has seen an increase in B2B disputes with the cannabis industry, including class action lawsuits that are being filed against hemp and CBD companies for false advertising, legal actions, and lawsuits between growers and dispensaries, and other business litigation.
If a Medical Marijuana Card holder purchases a firearm from a licensed firearm dealer, they will be required to complete an ATF form. This form requires the purchaser to admit to using federally illegal drugs. Without federal legalization laws in place, this now presents a dilemma for firearm purchasers who have the legal right to use Medical Marijuana in Utah.
Utah legislators did write provisions into HB 3001 that prohibit state law enforcement from spending any resources on trying to enforce gun laws, federal or otherwise. However, federal law enforcement, such as ATF officials, could still arrest you for possession of a firearm.
Yes, technically a federal official can arrest you for possession, even with a Medical Marijuana Card. However, a federal law has been enacted that the government cannot spend federal resources against people abiding by the state law.
Recently, U.S. Attorney General William Barr has faced backlash for an increased number of cannabis-related investigations, which in J.D.’s opinion, underscores why the federal government needs to implement legalization of marijuana.
When pulled over by the police, the protections of the Fifth Amendment provides you with no obligation to speak to answer their questions. You are only required to provide your license and registration.
J.D. recommends that if you are pulled over by police, roll down your window to a point where you can safely hand your license and your registration through to the officer. Next, ask the officer their reason for pulling you over. If you are asked any other questions from law enforcement about what you have been doing, where you have been, where I'm going, you can refuse to answer those questions.
At some point in the encounter, you should ask whether you are being detained or whether you're free to leave. If you're free to leave, it is a consensual encounter and you can drive away.
If you are being detained, you can invoke your Fifth Amendment right and then you have nothing more to say without legal counsel present.
If you're pulled over for a DUI, you do not have to consent to the field sobriety test. However, you do have to consent to a chemical test by getting a driver's license in Utah.
J.D. sees problems with law enforcement using the alcohol model of impairment to test for cannabis impairment. Some states have a limit in the certain amount of nanograms that can be in your blood. However, cannabis affects people differently.
So the way the law is written currently, you can still get a DUI if you are intoxicated. However, that leaves it up to officer interpretation, because there is no standard amount deemed to be intoxicating.
For Medical Cannabis patients, the law has an exception that they can have just cannabis metabolites in their system.
J.D. is a proponent of making law enforcement do their job and not volunteering any information to them.
It is important that you always have your Medical Marijuana Card with you in case you do encounter a situation with law enforcement. Also, if you are driving with cannabis in the vehicle, be sure to keep it in a locked case.
It is federally illegal to transport marijuana across state lines. However, under the state law until the end of this year, you can possess cannabis regardless of where you acquired it.
If you do purchase marijuana in an illegal way, law enforcement can still arrest you during the transaction. However, once you’re in possession, state law enforcement will not arrest you.
Starting January 1, 2021, all marijuana purchases must be done in-state at approved dispensaries.
J.D. recommends that patients use a lockable container. You are looking to make it difficult for others to access your Medical Marijuana products, similar to how opioids are put in child-proof containers.
Smoking is the most recognized way of ingesting cannabis. Telling patients that they are no longer able to smoke marijuana creates a problem. For example, a patient may have a letter or card, but in their car they have a pipe with resin in it. They will still be subject to criminal charges. Because this rule is in place, it opens up legal Medical Marijuana card holders to prosecution.
Patients in Utah can possess up to 113 grams of unprocessed flower, up to 20 grams of total THC.
There's no statute for this in the law, but the only people that are licensed to sell cannabis in Utah are the dispensaries.
You can call his office at (801)323-5000. You can also find him on the Christianson & Jensen website, on Twitter @utcannabislaw, or UTCannabisLaw.com.
Who is Katie Sly? [00:49]
Katie’s thoughts on the Utah Medical Marijuana experience for patients [05:41]
Will Medical Marijuana ever be covered by health insurance in Utah? [08:22]
How Tim sees his work evolving if Utah moves to legal recreational use [9:10]
More info about the use of open flames when consuming Medical Marijuana [10:45]
Katie’s thoughts on cannabis, Crohn’s disease, and hydration [25:02]
Results of Utah Therapeutic Health Center surveys [28:05]
Are patients noticing more benefits than they expected? [34:03]
What is the best way to consume cannabis for Crohn’s disease? [35:39]
A tip for reusing already vaporized herbs [40:26]
Tim’s education schedule [47:19]
Katie works at Utah Therapeutic Health Center and is the younger sister of Tim. Her primary role is to provide education and training to patients, including helping them with using the medicalcannabis.utah.gov/ site.
When Utah Therapeutic Health Center opened in March, there was an immediate demand for help in signing up for Medical Marijuana Cards. The first day, the team had a hundred missed calls. The Department of Health was not set up to provide Medical Cannabis to patients in a user-friendly way. Katie immediately joined the team to help with this demand.
Katie and Tim grew up in a conservative household. Her first experience with cannabis occurred in ninth grade.
As a sophomore, she went to a party where her and a friend consumed cannabis and alcohol. After getting caught, she was kicked off of her high school drill team.
In order to rejoin the drill team, she was told to no longer consume cannabis and to distance herself from her friend. She self describes as a “rule follower,” and complied with this.
Also during her sophomore year, she was diagnosed with Crohn’s disease, and had hundreds of kidney stones. To deal with the pain, a doctor prescribed her Lortab and told her to take it once per day.
She decided not to use the medication and, after visiting another doctor, had surgery to remove the kidney stones. This experience opened her eyes to the fact that opioids do not have to be the first choice for pain relief, and that there are often safer alternatives for treatment.
Many clinics are not set up to help their patients. Tim and Katie’s primary goal with Utah Therapeutic Health Center is to help the patients. Not just with handing out Medical Cannabis Cards, but ensuring that they stay connected with the patient.
The experience for patients to perform a 90-day renewal can be a frustrating one. Katie works to make this experience easier by helping patients adjust dosing, and making other recommendations for treatment.
The team has taken it upon themselves to be the primary educator for patients, which would typically be the state’s responsibility.
Tim has seen states, such as New York, begin to push insurance companies to cover the visits. Utah Therapeutic Health Center actually has a staff member who is credentialing for insurance to prepare for when Medical Marijuana would be covered by health insurance in Utah. He believes it will take a year or two before this occurs in Utah.
People have told time that if legalization occurs then they will be put out of business. However, Tim believes that Utah Therapeutic Health Center and UtahMarijuana.org will still be the experts that patients turn to for help. In fact, the majority of their patients are novice users, so there will still be a need for education and for expert help even if recreational use becomes legal.
When consuming Medical Marijuana in Utah, you are not allowed to consume using an open flame. Tim clarified this to say that combustion at a high temperature is the issue. For example, a car cigarette lighter does not have an open flame. However, it is the combustion at a high temperature that prevents patients from consuming Medical Marijuana with a joint or pipe.
For someone with Crohn's disease, or any digestion disease, Katie says that the best side effect of smoking cannabis is being thirsty. Typically with digestion diseases, doctors will recommend that patients stay hydrated. Because Medical Marijuana could cause you to become thirsty, a benefit of this side effect could be to encourage you to stay hydrated. Also, if you have issues with nausea, Medical Marijuana could help prevent vomiting when drinking water.
Utah Therapeutic Health Center sends 90-day surveys to better understand their patients’ experience by asking questions, such as “what are you using” and “what is working?”
About 100 patients have completed the survey. They are currently going through the data to identify patterns. One pattern they found is that patients are seeing a decrease in anxiety and insomnia.
The goal of these surveys is to use the information to better educate patients and provide more effective treatments. Also, they can use this data to help push legislators for updates to laws and qualifying conditions.
The data is always HIPAA compliant and secure. None of this data will be shared with anybody else and no personal identifying information is associated with the data.
Tim and Katie have noticed that patients are seeing other benefits of cannabis use, including reduced anxiety and improved sleep.
Tim compared plant treatments vs. traditional treatment via pharmaceuticals. With traditional treatments, doctors focus on one symptom, one treatment. For example, a poorly-functioning thyroid is treated with thyroid medication. But, there is not a focus on treating the whole patient.
Plant medicines not only help treat the immediate symptoms, but also provide additional benefits to treat the patient holistically.
Vaping, either with vape cartridges or a dry herb vaporizer, is a great way to consume cannabis because it is fast acting. Oral delivery could work better in some cases because it acts directly on the gut, but effects are not as immediate.
Once herbs are vaporized, the cannabinoid CBN is released. Katie received a tip from a patient to take already vaporized herbs from a dry herb vaporizer and sprinkle it on peanut butter toast. Tim has also heard from patients that they will reuse already vaporized herbs and sprinkle it on foods or bake it and turn it into an oil.
Tim will be speaking on July 16th at a CBD shop in Kaysville. Tim will also do a lecture in August that will be recorded.
Who is Mindy Madeo? [00:07]
Is Mindy connected with other pharmacists in the area? [9:00]
Mindy’s thoughts on having a pharmacist in a dispensary [12:39]
Does Mindy believe pharmacists should have personal experience with cannabis? [17:08]
What is the Wholesome Co. pharmacy like? [18:18]
How do consultations with pharmacists work? [20:00]
Mindy’s thoughts about dosing [29:18]
Mindy’s cannabis education [31:40]
When will the Wholesome Co. pharmacy open? [41:56]
How Mindy sees cannabis as part of a whole health plan [42:41]
Mindy is the pharmacist for Wholesome Co. After her education at the University of Utah, she worked as a retail pharmacist.
As a retail pharmacist, she became disillusioned with pharmacy practice in general. She felt that a lot of patients were over prescribed medications. The healthcare industry was only focused on treating symptoms and diseases with medication, and not looking at the whole patient.
She witnessed the progression of the current opioid epidemic and found it heartening to see patients prescribed massive doses of pain medications and watch their quality of life go down.
Mindy actually considered retirement about three years ago. However, in 2018 when Proposition 2 passed, she saw an opportunity to be involved with plant and herbal medicines.
She did everything she could to educate herself, including reading books, listening to podcasts, etc.
Wholesome Co. then reached out to her on LinkedIn to join their team. They connected early in the process, before they got their cultivation or their pharmacy license. Mindy felt they both have similar ideals about health and treatment.
Mindy is forming a group of pharmacists called Utah Cannabis Pharmacist Association. This group will be under the umbrella of the Utah Cannabis Association.
Pharmacists in the area have visited each other's pharmacies and sat in on consultations. Also, because cannabis pharmacists are a new role, it is important for everyone in this role to work together and define what the role means.
Mindy believes there is definitely a need for a pharmacist. Pharmacists have a background in pharmacokinetics, diseases, state management, etc. For every medication that exists, pharmacists are educated on the disease that it treats, the mechanism of the disease, and how it is diagnosed. As a result, pharmacists have a large, broad knowledge base that can be valuable for patients.
Most pharmacists aren't educated with cannabis. However, Mindy believes they can get educated on cannabis fairly quickly.
Mindy does not believe you need to have personal experience. It could be helpful, especially if you understand different strains. However, just as pharmacists do not need to have personal experience with blood pressure medication to properly prescribe it, a pharmacist does not have to consume cannabis.
It is next to Costco in Bountiful. They are still building the location. The location will have a large pharmacy and waiting area. Also, there will be consultation rooms for patients to talk to Mindy.
After patients receive their card, they will come to the Wholesome Co. pharmacy and have a consultation with Mindy.
Mindy has a list of questions she asks clients to better understand their conditions, experience with cannabis, and recommendations from their QMP. She also asks questions to learn more about their pain, including how severe the pain is, times of the day when pain is worse, and if any treatments have made the pain better.
To help prevent negative drug interactions with cannabis, Mindy will also review current medications the patient is using.
Mindy believes that a pharmacist shouldn’t dose a patient. The patient is dosing themselves. As pharmacists and medical providers, they are helping a patient determine the lowest dose needed to create an effect. The patient is the one who is in control of this, with the pharmacists and medical providers giving them the tools they need to learn to dose themselves.
When Mindy decided to get involved with the Medical Marijuana industry, she began looking for a good online education. She settled on a master's degree program in Cannabis, Science, and Therapeutics at the University of Maryland in Baltimore.
Mindy is hoping to be able to open on July 17th.
Mindy believes that, along with using cannabis to treat medical conditions, health professionals should also encourage a healthy lifestyle. She tells patients that it is wise to use cannabis, but to also exercise, practice meditation or journaling, and socialize with friends.
She also says that there isn’t a distinction between a recreational user and a medical user — both are using cannabis to be a healthier person. Even if you are that recreational user consuming cannabis to loosen up at a party, you are using it to relieve anxiety instead of a traditional anxiety medication.